Ali Jaan, Farhan Khalid, Abdullah M Firoze Ahmed, Ahmed Salman, Trisha Meghal, Doantrang Du
{"title":"吞噬血淋巴细胞增多症与胰腺癌症:罕见的关联。","authors":"Ali Jaan, Farhan Khalid, Abdullah M Firoze Ahmed, Ahmed Salman, Trisha Meghal, Doantrang Du","doi":"10.55729/2000-9666.1225","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Hemophagocytic lymphohistiocytosis (HLH) or hemophagocytic syndrome (HPS) is a life-threatening and relatively rare condition that usually presents as a multisystem febrile illness. It is associated with excessive activation of the immune system and hypercytokinemia, leading to an unregulated aggregation of macrophages and lymphocytes. Here, we present the first likely case of HLH with metastatic pancreatic carcinoma being the underlying etiology.</p><p><strong>Case: </strong>A 44-year-old male with past medical history significant for heart transplant for which he was on tacrolimus, End-Stage Renal Disease (ESRD) on hemodialysis, recently treated CMV viremia, and necrotizing pancreatitis presented to the emergency with complaints of chills, decreased appetite, worsening non-bloody emesis, and dull left upper quadrant abdominal pain with radiation to the back for four days. No shortness of breath, fever, diarrhea, or blood in the stool was reported. Vitals on admission were blood pressure of 90/61 mmHg, a heart rate of 110 beats per minute, temperature of 98.1 °F, and respiratory rate of 18 per minute. Physical exam was significant for scleral icterus, decreased bibasilar breath sounds, moderate abdominal tenderness in the left flank and left upper abdominal quadrant without any palpable mass, and 1+ bilateral pedal edema. The remainder of the physical examination was benign. Electrocardiogram (EKG) showed sinus tachycardia without any ischemic changes, and chest x-ray showed mild pulmonary edema. Initial blood workup revealed WBC at 8.3 k/uL, hemoglobin of 10.2 g/dL, platelet count of 90 k/uL, and BUN/creatinine of 45/5.8 (baseline 40/5.0). Cardiac workup showed an elevated high sensitivity troponin level of 2479 pg/mL and brain natriuretic peptide (BNP) of 600 (0-100 pg/mL). The hepatobiliary profile showed an aspartate transaminase (AST) level of 2645 U/L, an alanine transaminase (ALT) of 2935 U/L, alkaline phosphatase (ALP) of 106 U/L, and lipase of 61 U/L, with total and conjugated bilirubin of 3.5 mg/dL and 2.1 mg/dL, respectively. Transthoracic echocardiogram (TTE) showed reduced left ventricular size with hyperdynamic systolic function. Computerized tomography (CT) scan of the abdomen (Fig. 1) revealed numerous new pulmonary nodules, ring-enhancing lesions within the liver, hyperenhancement of the pancreas with walled-off necrosis, and splenomegaly. Microbiological work-up was positive for cytomegalovirus (CMV) serologies (IgM and IgG) but absent viral load on Polymerase Chain Reaction (PCR). The initial diagnosis was systemic inflammatory respiratory syndrome (SIRS), likely septic versus distributive in the setting of pancreatitis, demand mediated non-ST segment elevation myocardial infarction (NSTEMI), and shock liver. Tacrolimus was held, and the patient was started on broad-spectrum antibiotics including vancomycin and cefepime for sepsis of unknown origin along with vasopressors for hypotension, requiring admission to the medical intensive care unit. Blood and urine cultures were collected on admission which remained negative throughout the course of hospital. CA19-9 levels were found elevated at 5587 U/mL. Liver biopsy was consistent with poorly differentiated adenocarcinoma of pancreatic origin. Both Infectious Disease and Hematology were consulted due to broad differential diagnoses. Due to the patient's continued hemodynamic instability and nonresponsiveness to the antibiotics, HLH was suspected with supporting labs as follows: ferritin 55,740 ng/mL (22-322 ng/mL), triglycerides 177 mg/dL (30-150 mg/dL), and fibrinogen 244 mg/dL (173-454 mg/dL), thus conferring 70-80% probability of HPS based on H-score. Soluble IL-2 R levels came out at 19,188 pg/mL (ref range 175-858 pg/mL). The patient couldn't be started on HLH treatment due to initial concerns of underlying infection and the delay in results of soluble IL-2 Receptor (IL-2 R) levels. The infection as a possible etiology was ruled out due to negative blood and urine cultures and HLH was attributed to pancreatic cancer. A marrow biopsy couldn't be pursued as the patient died within a week of hospitalization. An autopsy was not performed as per family's request.</p><p><strong>Conclusion: </strong>HLH can occur secondary to solid cell malignancies including those from the pancreas and should be kept high in the differential in critically ill cancer patients who are nonresponsive to antibiotics. H-score has been reported to be a more sensitive tool compared to the HLH protocol, especially if used earlier during the presentation. Further research is needed to compare diagnostic efficacy for HLH protocol verses H-score especially in critically ill patients as they might benefit from steroid trial.</p>","PeriodicalId":15460,"journal":{"name":"Journal of Community Hospital Internal Medicine Perspectives","volume":"13 5","pages":"68-71"},"PeriodicalIF":0.9000,"publicationDate":"2023-09-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/46/79/jchim-13-05-068.PMC10589035.pdf","citationCount":"0","resultStr":"{\"title\":\"Hemophagocytic Lymphohistiocytosis and Pancreatic Cancer: A Rare Association.\",\"authors\":\"Ali Jaan, Farhan Khalid, Abdullah M Firoze Ahmed, Ahmed Salman, Trisha Meghal, Doantrang Du\",\"doi\":\"10.55729/2000-9666.1225\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Hemophagocytic lymphohistiocytosis (HLH) or hemophagocytic syndrome (HPS) is a life-threatening and relatively rare condition that usually presents as a multisystem febrile illness. It is associated with excessive activation of the immune system and hypercytokinemia, leading to an unregulated aggregation of macrophages and lymphocytes. Here, we present the first likely case of HLH with metastatic pancreatic carcinoma being the underlying etiology.</p><p><strong>Case: </strong>A 44-year-old male with past medical history significant for heart transplant for which he was on tacrolimus, End-Stage Renal Disease (ESRD) on hemodialysis, recently treated CMV viremia, and necrotizing pancreatitis presented to the emergency with complaints of chills, decreased appetite, worsening non-bloody emesis, and dull left upper quadrant abdominal pain with radiation to the back for four days. No shortness of breath, fever, diarrhea, or blood in the stool was reported. Vitals on admission were blood pressure of 90/61 mmHg, a heart rate of 110 beats per minute, temperature of 98.1 °F, and respiratory rate of 18 per minute. Physical exam was significant for scleral icterus, decreased bibasilar breath sounds, moderate abdominal tenderness in the left flank and left upper abdominal quadrant without any palpable mass, and 1+ bilateral pedal edema. The remainder of the physical examination was benign. Electrocardiogram (EKG) showed sinus tachycardia without any ischemic changes, and chest x-ray showed mild pulmonary edema. Initial blood workup revealed WBC at 8.3 k/uL, hemoglobin of 10.2 g/dL, platelet count of 90 k/uL, and BUN/creatinine of 45/5.8 (baseline 40/5.0). Cardiac workup showed an elevated high sensitivity troponin level of 2479 pg/mL and brain natriuretic peptide (BNP) of 600 (0-100 pg/mL). The hepatobiliary profile showed an aspartate transaminase (AST) level of 2645 U/L, an alanine transaminase (ALT) of 2935 U/L, alkaline phosphatase (ALP) of 106 U/L, and lipase of 61 U/L, with total and conjugated bilirubin of 3.5 mg/dL and 2.1 mg/dL, respectively. Transthoracic echocardiogram (TTE) showed reduced left ventricular size with hyperdynamic systolic function. Computerized tomography (CT) scan of the abdomen (Fig. 1) revealed numerous new pulmonary nodules, ring-enhancing lesions within the liver, hyperenhancement of the pancreas with walled-off necrosis, and splenomegaly. Microbiological work-up was positive for cytomegalovirus (CMV) serologies (IgM and IgG) but absent viral load on Polymerase Chain Reaction (PCR). The initial diagnosis was systemic inflammatory respiratory syndrome (SIRS), likely septic versus distributive in the setting of pancreatitis, demand mediated non-ST segment elevation myocardial infarction (NSTEMI), and shock liver. Tacrolimus was held, and the patient was started on broad-spectrum antibiotics including vancomycin and cefepime for sepsis of unknown origin along with vasopressors for hypotension, requiring admission to the medical intensive care unit. Blood and urine cultures were collected on admission which remained negative throughout the course of hospital. CA19-9 levels were found elevated at 5587 U/mL. Liver biopsy was consistent with poorly differentiated adenocarcinoma of pancreatic origin. Both Infectious Disease and Hematology were consulted due to broad differential diagnoses. Due to the patient's continued hemodynamic instability and nonresponsiveness to the antibiotics, HLH was suspected with supporting labs as follows: ferritin 55,740 ng/mL (22-322 ng/mL), triglycerides 177 mg/dL (30-150 mg/dL), and fibrinogen 244 mg/dL (173-454 mg/dL), thus conferring 70-80% probability of HPS based on H-score. Soluble IL-2 R levels came out at 19,188 pg/mL (ref range 175-858 pg/mL). The patient couldn't be started on HLH treatment due to initial concerns of underlying infection and the delay in results of soluble IL-2 Receptor (IL-2 R) levels. The infection as a possible etiology was ruled out due to negative blood and urine cultures and HLH was attributed to pancreatic cancer. A marrow biopsy couldn't be pursued as the patient died within a week of hospitalization. An autopsy was not performed as per family's request.</p><p><strong>Conclusion: </strong>HLH can occur secondary to solid cell malignancies including those from the pancreas and should be kept high in the differential in critically ill cancer patients who are nonresponsive to antibiotics. H-score has been reported to be a more sensitive tool compared to the HLH protocol, especially if used earlier during the presentation. Further research is needed to compare diagnostic efficacy for HLH protocol verses H-score especially in critically ill patients as they might benefit from steroid trial.</p>\",\"PeriodicalId\":15460,\"journal\":{\"name\":\"Journal of Community Hospital Internal Medicine Perspectives\",\"volume\":\"13 5\",\"pages\":\"68-71\"},\"PeriodicalIF\":0.9000,\"publicationDate\":\"2023-09-02\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/46/79/jchim-13-05-068.PMC10589035.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Community Hospital Internal Medicine Perspectives\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.55729/2000-9666.1225\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"MEDICINE, GENERAL & INTERNAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Community Hospital Internal Medicine Perspectives","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.55729/2000-9666.1225","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
Hemophagocytic Lymphohistiocytosis and Pancreatic Cancer: A Rare Association.
Introduction: Hemophagocytic lymphohistiocytosis (HLH) or hemophagocytic syndrome (HPS) is a life-threatening and relatively rare condition that usually presents as a multisystem febrile illness. It is associated with excessive activation of the immune system and hypercytokinemia, leading to an unregulated aggregation of macrophages and lymphocytes. Here, we present the first likely case of HLH with metastatic pancreatic carcinoma being the underlying etiology.
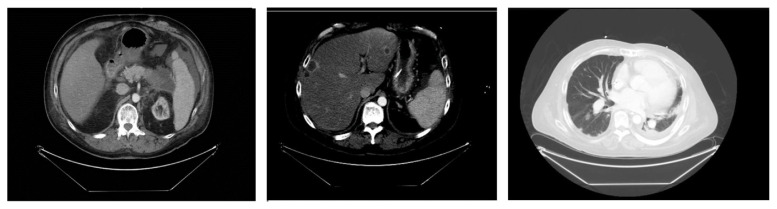
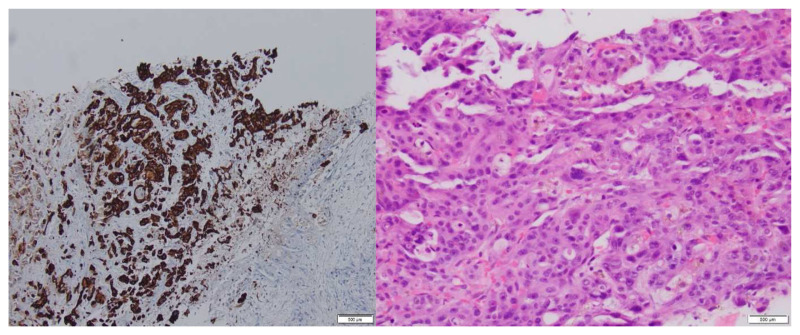
Case: A 44-year-old male with past medical history significant for heart transplant for which he was on tacrolimus, End-Stage Renal Disease (ESRD) on hemodialysis, recently treated CMV viremia, and necrotizing pancreatitis presented to the emergency with complaints of chills, decreased appetite, worsening non-bloody emesis, and dull left upper quadrant abdominal pain with radiation to the back for four days. No shortness of breath, fever, diarrhea, or blood in the stool was reported. Vitals on admission were blood pressure of 90/61 mmHg, a heart rate of 110 beats per minute, temperature of 98.1 °F, and respiratory rate of 18 per minute. Physical exam was significant for scleral icterus, decreased bibasilar breath sounds, moderate abdominal tenderness in the left flank and left upper abdominal quadrant without any palpable mass, and 1+ bilateral pedal edema. The remainder of the physical examination was benign. Electrocardiogram (EKG) showed sinus tachycardia without any ischemic changes, and chest x-ray showed mild pulmonary edema. Initial blood workup revealed WBC at 8.3 k/uL, hemoglobin of 10.2 g/dL, platelet count of 90 k/uL, and BUN/creatinine of 45/5.8 (baseline 40/5.0). Cardiac workup showed an elevated high sensitivity troponin level of 2479 pg/mL and brain natriuretic peptide (BNP) of 600 (0-100 pg/mL). The hepatobiliary profile showed an aspartate transaminase (AST) level of 2645 U/L, an alanine transaminase (ALT) of 2935 U/L, alkaline phosphatase (ALP) of 106 U/L, and lipase of 61 U/L, with total and conjugated bilirubin of 3.5 mg/dL and 2.1 mg/dL, respectively. Transthoracic echocardiogram (TTE) showed reduced left ventricular size with hyperdynamic systolic function. Computerized tomography (CT) scan of the abdomen (Fig. 1) revealed numerous new pulmonary nodules, ring-enhancing lesions within the liver, hyperenhancement of the pancreas with walled-off necrosis, and splenomegaly. Microbiological work-up was positive for cytomegalovirus (CMV) serologies (IgM and IgG) but absent viral load on Polymerase Chain Reaction (PCR). The initial diagnosis was systemic inflammatory respiratory syndrome (SIRS), likely septic versus distributive in the setting of pancreatitis, demand mediated non-ST segment elevation myocardial infarction (NSTEMI), and shock liver. Tacrolimus was held, and the patient was started on broad-spectrum antibiotics including vancomycin and cefepime for sepsis of unknown origin along with vasopressors for hypotension, requiring admission to the medical intensive care unit. Blood and urine cultures were collected on admission which remained negative throughout the course of hospital. CA19-9 levels were found elevated at 5587 U/mL. Liver biopsy was consistent with poorly differentiated adenocarcinoma of pancreatic origin. Both Infectious Disease and Hematology were consulted due to broad differential diagnoses. Due to the patient's continued hemodynamic instability and nonresponsiveness to the antibiotics, HLH was suspected with supporting labs as follows: ferritin 55,740 ng/mL (22-322 ng/mL), triglycerides 177 mg/dL (30-150 mg/dL), and fibrinogen 244 mg/dL (173-454 mg/dL), thus conferring 70-80% probability of HPS based on H-score. Soluble IL-2 R levels came out at 19,188 pg/mL (ref range 175-858 pg/mL). The patient couldn't be started on HLH treatment due to initial concerns of underlying infection and the delay in results of soluble IL-2 Receptor (IL-2 R) levels. The infection as a possible etiology was ruled out due to negative blood and urine cultures and HLH was attributed to pancreatic cancer. A marrow biopsy couldn't be pursued as the patient died within a week of hospitalization. An autopsy was not performed as per family's request.
Conclusion: HLH can occur secondary to solid cell malignancies including those from the pancreas and should be kept high in the differential in critically ill cancer patients who are nonresponsive to antibiotics. H-score has been reported to be a more sensitive tool compared to the HLH protocol, especially if used earlier during the presentation. Further research is needed to compare diagnostic efficacy for HLH protocol verses H-score especially in critically ill patients as they might benefit from steroid trial.
期刊介绍:
JCHIMP provides: up-to-date information in the field of Internal Medicine to community hospital medical professionals a platform for clinical faculty, residents, and medical students to publish research relevant to community hospital programs. Manuscripts that explore aspects of medicine at community hospitals welcome, including but not limited to: the best practices of community academic programs community hospital-based research opinion and insight from community hospital leadership and faculty the scholarly work of residents and medical students affiliated with community hospitals.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


