Shin-Jae Kim, Pratyush Shahi, Sang-Ho Lee, Junseok Bae
{"title":"颈椎前路多节段截骨和后路内固定治疗颈椎后凸性骨髓病的远期疗效。","authors":"Shin-Jae Kim, Pratyush Shahi, Sang-Ho Lee, Junseok Bae","doi":"10.14245/ns.2550256.128","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>To analyze long-term clinical and radiological outcomes after multilevel anterior osteotomy with posterior instrumentation in patients with ossification of posterior longitudinal ligament (OPLL)-induced myelopathy and cervical kyphosis.</p><p><strong>Methods: </strong>Patients who underwent multilevel anterior osteotomy with posterior instrumentation for OPLL-induced myelopathy and cervical kyphosis and had a minimum of 5-year follow-up were included. Clinical outcomes (Japanese Orthopaedic Association score system for cervical myelopathy [C-JOA], 12-item Short Form health survey [SF-12], Neck Disability Index [NDI]) and radiological parameters (C2-7 lordosis, center of gravity of the head [CGH]-C7 sagittal vertical axis [SVA], T1 slope) were analyzed at the preoperative, immediate postoperative, and latest follow-up timepoints.</p><p><strong>Results: </strong>Twenty-eight patients were included. The average follow-up period was 66.4 months. All clinical outcome parameters showed significant improvement. C-JOA, SF-12, and NDI showed significant improvement at latest follow-up (p<0.001). C2-7 lordosis increased significantly immediately postoperatively (-6.0°±10.4°) compared to preoperatively (+9.2°±9.6°), and was largely maintained at latest follow-up (-5.7°±9.4°). T1 slope significantly increased between the immediate postoperative timepoint (21.9°±7.7°) and latest follow-up (24.2°±9.5°) (p=0.046). CGH-C7 SVA significantly increased between the immediate postoperative timepoint (22.7±14.8 mm) and latest follow-up (32.2±22.6 mm) (p=0.046).</p><p><strong>Conclusion: </strong>Multilevel anterior osteotomy with posterior instrumentation is a safe and effective surgical option for OPLL-induced myelopathy with kyphotic cervical alignment. Future studies are required to investigate the forward tilting of cervical spine over time after surgery.</p>","PeriodicalId":19269,"journal":{"name":"Neurospine","volume":"22 3","pages":"623-630"},"PeriodicalIF":3.6000,"publicationDate":"2025-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12518910/pdf/","citationCount":"0","resultStr":"{\"title\":\"Long-term Outcomes of Multilevel Anterior Cervical Osteotomy and Posterior Instrumentation for OPLL-Induced Myelopathy With Cervical Kyphosis.\",\"authors\":\"Shin-Jae Kim, Pratyush Shahi, Sang-Ho Lee, Junseok Bae\",\"doi\":\"10.14245/ns.2550256.128\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>To analyze long-term clinical and radiological outcomes after multilevel anterior osteotomy with posterior instrumentation in patients with ossification of posterior longitudinal ligament (OPLL)-induced myelopathy and cervical kyphosis.</p><p><strong>Methods: </strong>Patients who underwent multilevel anterior osteotomy with posterior instrumentation for OPLL-induced myelopathy and cervical kyphosis and had a minimum of 5-year follow-up were included. Clinical outcomes (Japanese Orthopaedic Association score system for cervical myelopathy [C-JOA], 12-item Short Form health survey [SF-12], Neck Disability Index [NDI]) and radiological parameters (C2-7 lordosis, center of gravity of the head [CGH]-C7 sagittal vertical axis [SVA], T1 slope) were analyzed at the preoperative, immediate postoperative, and latest follow-up timepoints.</p><p><strong>Results: </strong>Twenty-eight patients were included. The average follow-up period was 66.4 months. All clinical outcome parameters showed significant improvement. C-JOA, SF-12, and NDI showed significant improvement at latest follow-up (p<0.001). C2-7 lordosis increased significantly immediately postoperatively (-6.0°±10.4°) compared to preoperatively (+9.2°±9.6°), and was largely maintained at latest follow-up (-5.7°±9.4°). T1 slope significantly increased between the immediate postoperative timepoint (21.9°±7.7°) and latest follow-up (24.2°±9.5°) (p=0.046). CGH-C7 SVA significantly increased between the immediate postoperative timepoint (22.7±14.8 mm) and latest follow-up (32.2±22.6 mm) (p=0.046).</p><p><strong>Conclusion: </strong>Multilevel anterior osteotomy with posterior instrumentation is a safe and effective surgical option for OPLL-induced myelopathy with kyphotic cervical alignment. Future studies are required to investigate the forward tilting of cervical spine over time after surgery.</p>\",\"PeriodicalId\":19269,\"journal\":{\"name\":\"Neurospine\",\"volume\":\"22 3\",\"pages\":\"623-630\"},\"PeriodicalIF\":3.6000,\"publicationDate\":\"2025-09-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12518910/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Neurospine\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.14245/ns.2550256.128\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/9/30 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q1\",\"JCRName\":\"CLINICAL NEUROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Neurospine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.14245/ns.2550256.128","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/9/30 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
Long-term Outcomes of Multilevel Anterior Cervical Osteotomy and Posterior Instrumentation for OPLL-Induced Myelopathy With Cervical Kyphosis.
Objective: To analyze long-term clinical and radiological outcomes after multilevel anterior osteotomy with posterior instrumentation in patients with ossification of posterior longitudinal ligament (OPLL)-induced myelopathy and cervical kyphosis.
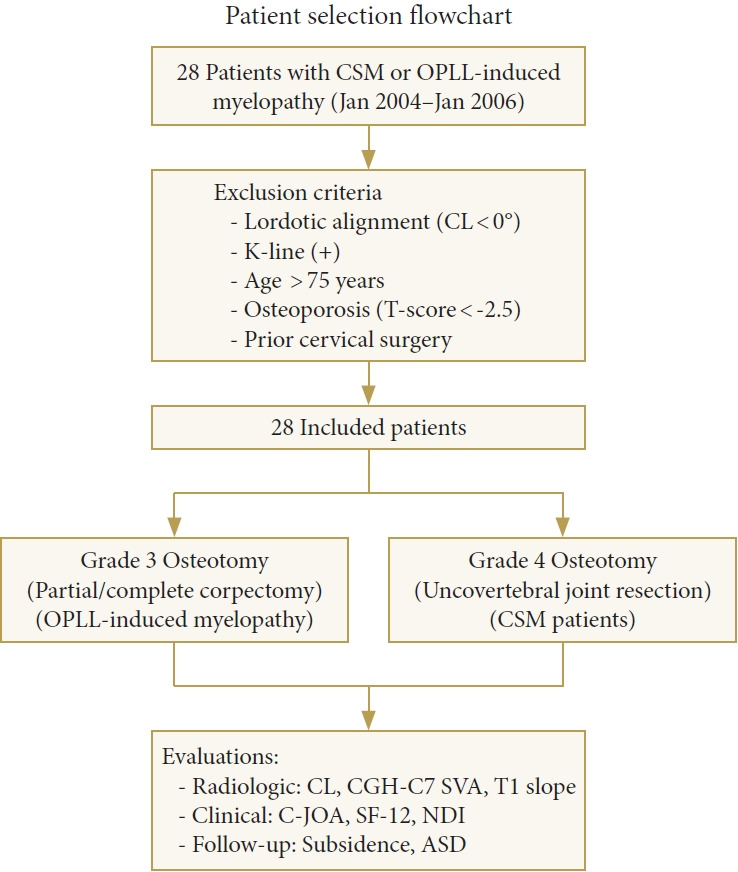
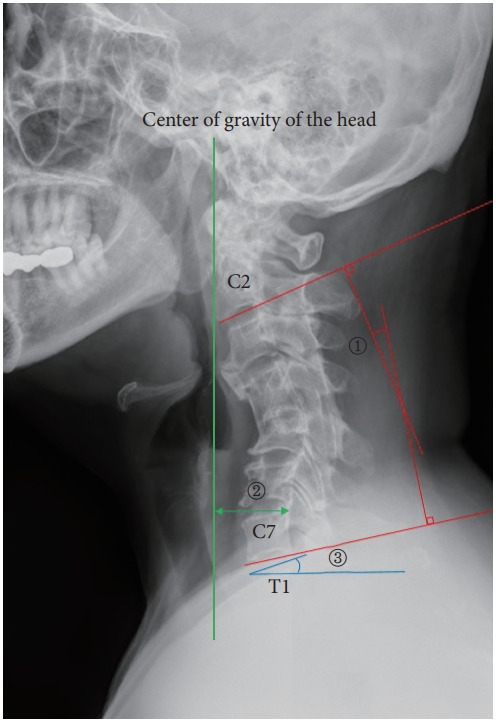
Methods: Patients who underwent multilevel anterior osteotomy with posterior instrumentation for OPLL-induced myelopathy and cervical kyphosis and had a minimum of 5-year follow-up were included. Clinical outcomes (Japanese Orthopaedic Association score system for cervical myelopathy [C-JOA], 12-item Short Form health survey [SF-12], Neck Disability Index [NDI]) and radiological parameters (C2-7 lordosis, center of gravity of the head [CGH]-C7 sagittal vertical axis [SVA], T1 slope) were analyzed at the preoperative, immediate postoperative, and latest follow-up timepoints.
Results: Twenty-eight patients were included. The average follow-up period was 66.4 months. All clinical outcome parameters showed significant improvement. C-JOA, SF-12, and NDI showed significant improvement at latest follow-up (p<0.001). C2-7 lordosis increased significantly immediately postoperatively (-6.0°±10.4°) compared to preoperatively (+9.2°±9.6°), and was largely maintained at latest follow-up (-5.7°±9.4°). T1 slope significantly increased between the immediate postoperative timepoint (21.9°±7.7°) and latest follow-up (24.2°±9.5°) (p=0.046). CGH-C7 SVA significantly increased between the immediate postoperative timepoint (22.7±14.8 mm) and latest follow-up (32.2±22.6 mm) (p=0.046).
Conclusion: Multilevel anterior osteotomy with posterior instrumentation is a safe and effective surgical option for OPLL-induced myelopathy with kyphotic cervical alignment. Future studies are required to investigate the forward tilting of cervical spine over time after surgery.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


