Rasha S Farag, Aditya S Kalluri, Geetha Iyer, Jennifer P Stevens, Carly E Milliren, James Brian McAlvin
{"title":"右美托咪定治疗呼吸道合胞病毒细支气管炎患儿临床显著性心动过缓:机械通气改善效果。","authors":"Rasha S Farag, Aditya S Kalluri, Geetha Iyer, Jennifer P Stevens, Carly E Milliren, James Brian McAlvin","doi":"10.1136/bmjpo-2025-003625","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Limited evidence exists on the additive risk of bradycardia in children with respiratory syncytial virus (RSV) bronchiolitis receiving dexmedetomidine (DMED). We aim to study the association between RSV bronchiolitis and bradycardia during DMED administration.</p><p><strong>Methods: </strong>This retrospective cohort study included 273 children under 2 years old admitted to the intensive care units at Boston Children's Hospital with severe bronchiolitis and sedated with DMED from 2009 to 2022. Children were classified as RSV or non-RSV based on confirmed laboratory results. The primary outcome was a composite measure of clinically significant bradycardia, defined as either a heart rate <60 beats per minute or need for medical intervention(s). The secondary outcome was the minimum heart rate after DMED initiation. Subgroup analyses assessed potential effect modification by age, DMED doses, ventilation mode and pre- versus post-COVID-19.</p><p><strong>Results: </strong>The median (Q1, Q3) age was 8.0 (4.0, 13.7) months. Of the children studied, 85 (31.1%) had RSV bronchiolitis and 170 (62.3%) underwent invasive mechanical ventilation (IMV) at DMED initiation. Clinically significant bradycardia was observed in 71 (26.0%) patients with no significant difference between the RSV and non-RSV cohorts (OR: 1.80; 95% CI: 0.95 to 3.39; p = 0.07). Subgroup analyses showed effect modification with an increased likelihood of clinically significant bradycardia in the RSV group undergoing IMV (OR: 2.99 vs 0.45; Χ<sup>2</sup> <sub>1</sub>=3.6, p=0.04) or admitted before the COVID-19 pandemic (OR: 2.94 vs 0.51; Χ<sup>2</sup> <sub>1</sub>=4.7, p=0.03). The RSV cohort experienced a significantly greater heart rate reduction after DMED initiation (-8.07 bpm; 95% CI: -13.71 to -2.43; p = 0.005).</p><p><strong>Conclusions: </strong>Children with RSV bronchiolitis experienced greater heart rate reduction after DMED initiation, with a higher likelihood of clinically significant bradycardia if IMV is in use at DMED initiation or if admitted before the COVID-19 pandemic. Caution is warranted when treating RSV bronchiolitis patients with DMED.</p>","PeriodicalId":9069,"journal":{"name":"BMJ Paediatrics Open","volume":"9 1","pages":""},"PeriodicalIF":2.3000,"publicationDate":"2025-09-08","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12421169/pdf/","citationCount":"0","resultStr":"{\"title\":\"Clinically significant bradycardia in children with respiratory syncytial virus bronchiolitis receiving dexmedetomidine: effect modification by mechanical ventilation.\",\"authors\":\"Rasha S Farag, Aditya S Kalluri, Geetha Iyer, Jennifer P Stevens, Carly E Milliren, James Brian McAlvin\",\"doi\":\"10.1136/bmjpo-2025-003625\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Limited evidence exists on the additive risk of bradycardia in children with respiratory syncytial virus (RSV) bronchiolitis receiving dexmedetomidine (DMED). We aim to study the association between RSV bronchiolitis and bradycardia during DMED administration.</p><p><strong>Methods: </strong>This retrospective cohort study included 273 children under 2 years old admitted to the intensive care units at Boston Children's Hospital with severe bronchiolitis and sedated with DMED from 2009 to 2022. Children were classified as RSV or non-RSV based on confirmed laboratory results. The primary outcome was a composite measure of clinically significant bradycardia, defined as either a heart rate <60 beats per minute or need for medical intervention(s). The secondary outcome was the minimum heart rate after DMED initiation. Subgroup analyses assessed potential effect modification by age, DMED doses, ventilation mode and pre- versus post-COVID-19.</p><p><strong>Results: </strong>The median (Q1, Q3) age was 8.0 (4.0, 13.7) months. Of the children studied, 85 (31.1%) had RSV bronchiolitis and 170 (62.3%) underwent invasive mechanical ventilation (IMV) at DMED initiation. Clinically significant bradycardia was observed in 71 (26.0%) patients with no significant difference between the RSV and non-RSV cohorts (OR: 1.80; 95% CI: 0.95 to 3.39; p = 0.07). Subgroup analyses showed effect modification with an increased likelihood of clinically significant bradycardia in the RSV group undergoing IMV (OR: 2.99 vs 0.45; Χ<sup>2</sup> <sub>1</sub>=3.6, p=0.04) or admitted before the COVID-19 pandemic (OR: 2.94 vs 0.51; Χ<sup>2</sup> <sub>1</sub>=4.7, p=0.03). The RSV cohort experienced a significantly greater heart rate reduction after DMED initiation (-8.07 bpm; 95% CI: -13.71 to -2.43; p = 0.005).</p><p><strong>Conclusions: </strong>Children with RSV bronchiolitis experienced greater heart rate reduction after DMED initiation, with a higher likelihood of clinically significant bradycardia if IMV is in use at DMED initiation or if admitted before the COVID-19 pandemic. Caution is warranted when treating RSV bronchiolitis patients with DMED.</p>\",\"PeriodicalId\":9069,\"journal\":{\"name\":\"BMJ Paediatrics Open\",\"volume\":\"9 1\",\"pages\":\"\"},\"PeriodicalIF\":2.3000,\"publicationDate\":\"2025-09-08\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12421169/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"BMJ Paediatrics Open\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1136/bmjpo-2025-003625\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"PEDIATRICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMJ Paediatrics Open","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1136/bmjpo-2025-003625","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"PEDIATRICS","Score":null,"Total":0}
引用次数: 0
摘要
背景:有限的证据表明,接受右美托咪定(DMED)治疗的呼吸道合胞病毒(RSV)毛细支气管炎患儿发生心动过缓的附加风险。我们的目的是研究RSV细支气管炎与DMED用药期间心动过缓的关系。方法:本回顾性队列研究纳入了2009年至2022年在波士顿儿童医院重症监护室接受DMED镇静治疗的273名2岁以下重症细支气管炎患儿。根据确认的实验室结果将儿童分为RSV或非RSV。主要终点是临床显著性心动过缓的综合指标,定义为心率。结果:中位(Q1, Q3)年龄为8.0(4.0,13.7)个月。在研究的儿童中,85名(31.1%)患有RSV细支气管炎,170名(62.3%)在DMED开始时接受了有创机械通气(IMV)。71例(26.0%)患者出现临床显著性心动过缓,RSV组与非RSV组之间无显著差异(OR: 1.80; 95% CI: 0.95 ~ 3.39; p = 0.07)。亚组分析显示,RSV组接受IMV治疗(OR: 2.99 vs 0.45; Χ2 1=3.6, p=0.04)或在COVID-19大流行前入院的患者发生临床显著性心动过缓的可能性增加(OR: 2.94 vs 0.51; Χ2 1=4.7, p=0.03),效果有所改善。RSV队列在DMED开始后经历了更大的心率降低(-8.07 bpm; 95% CI: -13.71至-2.43;p = 0.005)。结论:RSV毛细支气管炎患儿在DMED启动后出现更大的心率降低,如果在DMED启动时使用IMV或在COVID-19大流行前入院,则更有可能出现临床显著性心动过缓。在用DMED治疗RSV细支气管炎患者时要谨慎。
Clinically significant bradycardia in children with respiratory syncytial virus bronchiolitis receiving dexmedetomidine: effect modification by mechanical ventilation.
Background: Limited evidence exists on the additive risk of bradycardia in children with respiratory syncytial virus (RSV) bronchiolitis receiving dexmedetomidine (DMED). We aim to study the association between RSV bronchiolitis and bradycardia during DMED administration.
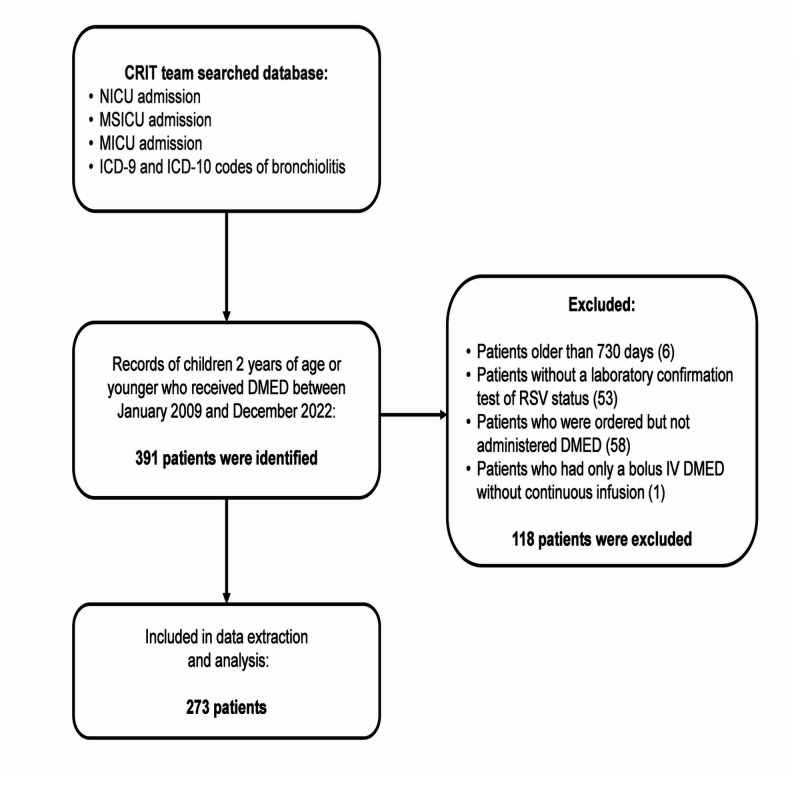
Methods: This retrospective cohort study included 273 children under 2 years old admitted to the intensive care units at Boston Children's Hospital with severe bronchiolitis and sedated with DMED from 2009 to 2022. Children were classified as RSV or non-RSV based on confirmed laboratory results. The primary outcome was a composite measure of clinically significant bradycardia, defined as either a heart rate <60 beats per minute or need for medical intervention(s). The secondary outcome was the minimum heart rate after DMED initiation. Subgroup analyses assessed potential effect modification by age, DMED doses, ventilation mode and pre- versus post-COVID-19.
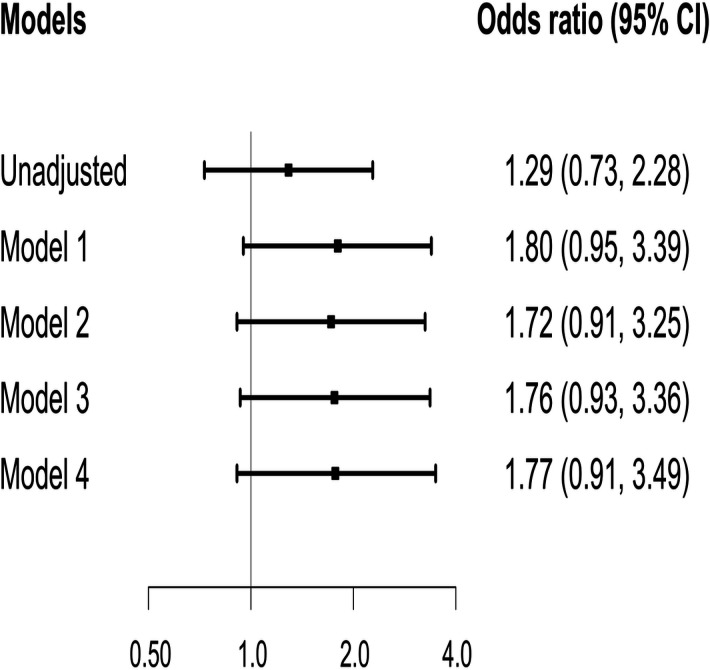
Results: The median (Q1, Q3) age was 8.0 (4.0, 13.7) months. Of the children studied, 85 (31.1%) had RSV bronchiolitis and 170 (62.3%) underwent invasive mechanical ventilation (IMV) at DMED initiation. Clinically significant bradycardia was observed in 71 (26.0%) patients with no significant difference between the RSV and non-RSV cohorts (OR: 1.80; 95% CI: 0.95 to 3.39; p = 0.07). Subgroup analyses showed effect modification with an increased likelihood of clinically significant bradycardia in the RSV group undergoing IMV (OR: 2.99 vs 0.45; Χ21=3.6, p=0.04) or admitted before the COVID-19 pandemic (OR: 2.94 vs 0.51; Χ21=4.7, p=0.03). The RSV cohort experienced a significantly greater heart rate reduction after DMED initiation (-8.07 bpm; 95% CI: -13.71 to -2.43; p = 0.005).
Conclusions: Children with RSV bronchiolitis experienced greater heart rate reduction after DMED initiation, with a higher likelihood of clinically significant bradycardia if IMV is in use at DMED initiation or if admitted before the COVID-19 pandemic. Caution is warranted when treating RSV bronchiolitis patients with DMED.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


