Paula A Jaimes-Buitron, Nicole Adams, Nan Kong, Carolina Vivas-Valencia
{"title":"2015 - 2019年印第安纳州阿片类药物处方时空分析","authors":"Paula A Jaimes-Buitron, Nicole Adams, Nan Kong, Carolina Vivas-Valencia","doi":"10.1186/s13011-025-00664-8","DOIUrl":null,"url":null,"abstract":"<p><p>People living in rural communities are more likely to receive opioid prescriptions, partly due to job-related injuries. State-level interventions have reduced opioid prescribing; however, rural/urban disparities persist due to differences in demographics and prescribing practices, particularly in states with large rural populations like Indiana. While spatiotemporal analyses have explored aspects of the opioid crisis, spatiotemporal patterns of opioid prescribing have not been sufficiently studied. This study utilizes a sample of Medicaid claims data from the Indiana Family and Social Services Administration from 2015 to 2019 to analyze spatiotemporal patterns of patients receiving at least one opioid prescription across Indiana. The goal was to analyze patient demographics and track prescription hotspot movement over time in rural and urban areas. We analyzed data for 107,574 Medicaid enrollees who received opioid prescriptions during the study period. We found that most patients in the cohort resided in urban areas, with the number of patients who were prescribed opioids and resided in rural areas decreasing at a faster rate. We conducted a negative binomial regression analysis to examine the relationship between various demographics (sex, age, race/ethnicity, and urban/rural classification) and the number of patients receiving at least one opioid prescription over time. Our findings indicate that older patients, patients identifying as females, patients who identify as White, and patients living in urban areas, are more likely to receive at least one opioid prescription. Additionally, the interaction effects revealed that patients from all demographic groups were more likely to receive at least one opioid prescription if they lived in urban areas, compared to those living in rural areas. Using Local Moran's I as a local spatial autocorrelation measure, we identified clusters highlighting transitions from rural to urban areas over time. In 2015-2016, three significant clusters emerged within rural-surrounded 3-digit ZIP codes (472, 474, 476), based on the Rural-Urban Commuting Area Codes. Over time, significant clusters shifted towards urban or mixed areas, possibly influenced by state guidelines and legislation. These findings enhance the understanding of opioid prescription dynamics and identify patterns in opioid prescribing rates in terms of the proportion of patients receiving opioid prescriptions among urban vs. rural communities in Indiana.</p>","PeriodicalId":22041,"journal":{"name":"Substance Abuse Treatment, Prevention, and Policy","volume":"20 1","pages":"30"},"PeriodicalIF":3.0000,"publicationDate":"2025-08-08","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12335077/pdf/","citationCount":"0","resultStr":"{\"title\":\"A spatiotemporal analysis of opioid prescriptions in Indiana from 2015 to 2019.\",\"authors\":\"Paula A Jaimes-Buitron, Nicole Adams, Nan Kong, Carolina Vivas-Valencia\",\"doi\":\"10.1186/s13011-025-00664-8\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>People living in rural communities are more likely to receive opioid prescriptions, partly due to job-related injuries. State-level interventions have reduced opioid prescribing; however, rural/urban disparities persist due to differences in demographics and prescribing practices, particularly in states with large rural populations like Indiana. While spatiotemporal analyses have explored aspects of the opioid crisis, spatiotemporal patterns of opioid prescribing have not been sufficiently studied. This study utilizes a sample of Medicaid claims data from the Indiana Family and Social Services Administration from 2015 to 2019 to analyze spatiotemporal patterns of patients receiving at least one opioid prescription across Indiana. The goal was to analyze patient demographics and track prescription hotspot movement over time in rural and urban areas. We analyzed data for 107,574 Medicaid enrollees who received opioid prescriptions during the study period. We found that most patients in the cohort resided in urban areas, with the number of patients who were prescribed opioids and resided in rural areas decreasing at a faster rate. We conducted a negative binomial regression analysis to examine the relationship between various demographics (sex, age, race/ethnicity, and urban/rural classification) and the number of patients receiving at least one opioid prescription over time. Our findings indicate that older patients, patients identifying as females, patients who identify as White, and patients living in urban areas, are more likely to receive at least one opioid prescription. Additionally, the interaction effects revealed that patients from all demographic groups were more likely to receive at least one opioid prescription if they lived in urban areas, compared to those living in rural areas. Using Local Moran's I as a local spatial autocorrelation measure, we identified clusters highlighting transitions from rural to urban areas over time. In 2015-2016, three significant clusters emerged within rural-surrounded 3-digit ZIP codes (472, 474, 476), based on the Rural-Urban Commuting Area Codes. Over time, significant clusters shifted towards urban or mixed areas, possibly influenced by state guidelines and legislation. These findings enhance the understanding of opioid prescription dynamics and identify patterns in opioid prescribing rates in terms of the proportion of patients receiving opioid prescriptions among urban vs. rural communities in Indiana.</p>\",\"PeriodicalId\":22041,\"journal\":{\"name\":\"Substance Abuse Treatment, Prevention, and Policy\",\"volume\":\"20 1\",\"pages\":\"30\"},\"PeriodicalIF\":3.0000,\"publicationDate\":\"2025-08-08\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12335077/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Substance Abuse Treatment, Prevention, and Policy\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1186/s13011-025-00664-8\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"SUBSTANCE ABUSE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Substance Abuse Treatment, Prevention, and Policy","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s13011-025-00664-8","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"SUBSTANCE ABUSE","Score":null,"Total":0}
A spatiotemporal analysis of opioid prescriptions in Indiana from 2015 to 2019.
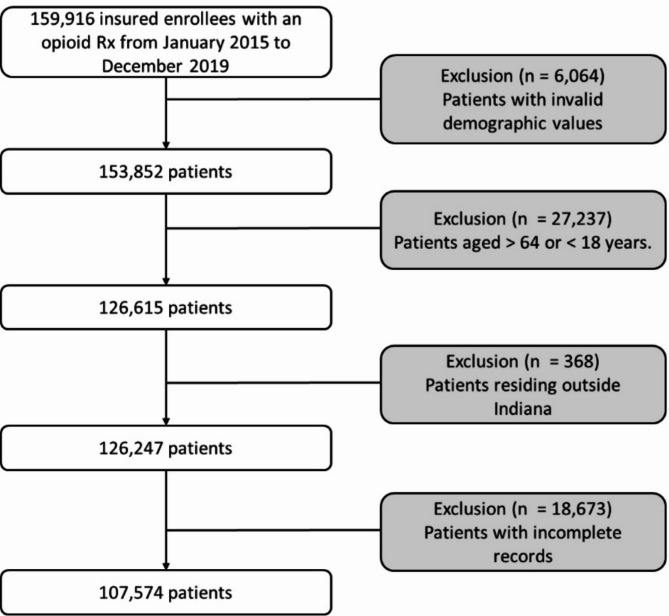
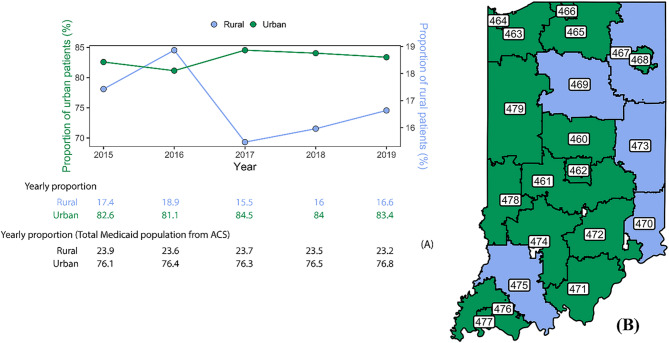
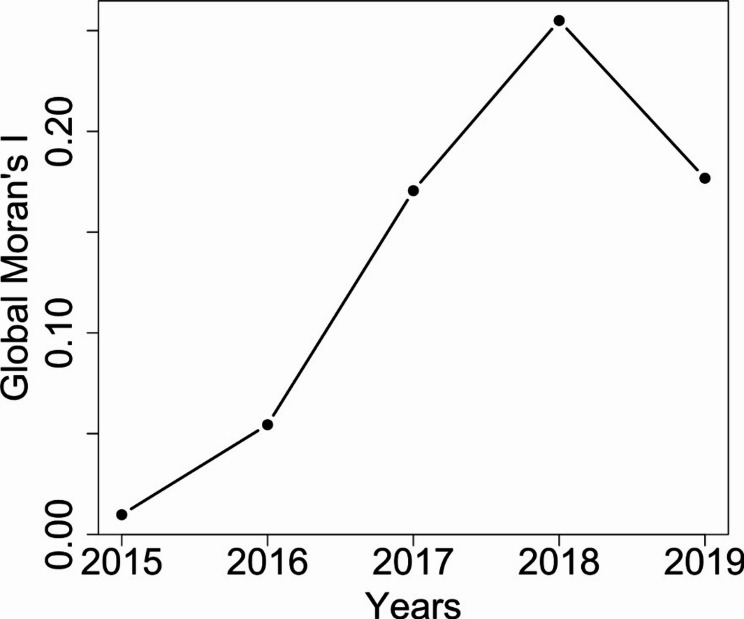
People living in rural communities are more likely to receive opioid prescriptions, partly due to job-related injuries. State-level interventions have reduced opioid prescribing; however, rural/urban disparities persist due to differences in demographics and prescribing practices, particularly in states with large rural populations like Indiana. While spatiotemporal analyses have explored aspects of the opioid crisis, spatiotemporal patterns of opioid prescribing have not been sufficiently studied. This study utilizes a sample of Medicaid claims data from the Indiana Family and Social Services Administration from 2015 to 2019 to analyze spatiotemporal patterns of patients receiving at least one opioid prescription across Indiana. The goal was to analyze patient demographics and track prescription hotspot movement over time in rural and urban areas. We analyzed data for 107,574 Medicaid enrollees who received opioid prescriptions during the study period. We found that most patients in the cohort resided in urban areas, with the number of patients who were prescribed opioids and resided in rural areas decreasing at a faster rate. We conducted a negative binomial regression analysis to examine the relationship between various demographics (sex, age, race/ethnicity, and urban/rural classification) and the number of patients receiving at least one opioid prescription over time. Our findings indicate that older patients, patients identifying as females, patients who identify as White, and patients living in urban areas, are more likely to receive at least one opioid prescription. Additionally, the interaction effects revealed that patients from all demographic groups were more likely to receive at least one opioid prescription if they lived in urban areas, compared to those living in rural areas. Using Local Moran's I as a local spatial autocorrelation measure, we identified clusters highlighting transitions from rural to urban areas over time. In 2015-2016, three significant clusters emerged within rural-surrounded 3-digit ZIP codes (472, 474, 476), based on the Rural-Urban Commuting Area Codes. Over time, significant clusters shifted towards urban or mixed areas, possibly influenced by state guidelines and legislation. These findings enhance the understanding of opioid prescription dynamics and identify patterns in opioid prescribing rates in terms of the proportion of patients receiving opioid prescriptions among urban vs. rural communities in Indiana.
期刊介绍:
Substance Abuse Treatment, Prevention, and Policy is an open access, peer-reviewed journal that encompasses research concerning substance abuse, with a focus on policy issues. The journal aims to provide an environment for the exchange of ideas, new research, consensus papers, and critical reviews, to bridge the established fields that share a mutual goal of reducing the harms from substance use. These fields include: legislation pertaining to substance use; correctional supervision of people with substance use disorder; medical treatment and screening; mental health services; research; and evaluation of substance use disorder programs.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


