{"title":"早期有针对性的基于风险的动脉导管未闭管理是否能改善早产儿的预后?来自观察性研究的见解。","authors":"Rachel Mullaly, Aisling Smith, Claire Murphy, Sean Armstrong, Lyudmyla Zakharchenko, Orla Franklin, Naomi McCallion, Afif El-Khuffash","doi":"10.1136/bmjpo-2025-003347","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>This study evaluates the outcomes of an early-targeted patent ductus arteriosus (PDA) management strategy in preterm infants using the EL-Khuffash PDA Severity Score (PDAsc) for risk stratification. The objective was to compare outcomes between high- and low-risk infants from an early-targeted treatment epoch and a historical reference epoch who were risk stratified but did not undergo treatment.</p><p><strong>Methods: </strong>We conducted a single-centre, observational cohort study in a level III neonatal intensive care unit. Infants born <29 weeks gestation were stratified into high- and low-risk groups using the PDAsc. High-risk infants in the early-targeted treatment epoch received medical intervention, while low-risk infants did not. Outcomes from this epoch were compared with a historical reference epoch in which risk was assigned but treatment was not implemented. The primary outcomes included chronic lung disease (CLD), ventilation days and oxygen days.</p><p><strong>Results: </strong>A total of 110 high-risk and 74 low-risk infants were identified in the early-targeted epoch, compared with 84 high-risk and 51 low-risk infants in the reference epoch. High-risk infants in the early-targeted treatment epoch who achieved successful PDA closure demonstrated fewer ventilation days (median 5 vs 11), fewer oxygen days (median 45 vs 65) and a lower incidence of CLD (59% vs 76%) compared with high-risk infants in the reference epoch. However, high-risk infants in the early-targeted treatment epoch who failed treatment experienced outcomes similar to high-risk infants in the reference epoch. Low-risk infants in both epochs exhibited comparable favourable outcomes.</p><p><strong>Conclusions: </strong>The implementation of early-targeted risk-based PDA management may be associated with improved respiratory outcomes in high-risk infants who successfully responded to treatment. However, the observational nature of this study limits causal inferences. These findings underscore the need for further research, including randomised controlled trials with improved patient selection, to better understand the relationship between stratified treatment and important outcomes.</p>","PeriodicalId":9069,"journal":{"name":"BMJ Paediatrics Open","volume":"9 1","pages":""},"PeriodicalIF":2.3000,"publicationDate":"2025-07-16","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12273076/pdf/","citationCount":"0","resultStr":"{\"title\":\"Does early-targeted risk-based management of a patent ductus arteriosus improve outcomes in preterm infants? Insights from an observational study.\",\"authors\":\"Rachel Mullaly, Aisling Smith, Claire Murphy, Sean Armstrong, Lyudmyla Zakharchenko, Orla Franklin, Naomi McCallion, Afif El-Khuffash\",\"doi\":\"10.1136/bmjpo-2025-003347\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>This study evaluates the outcomes of an early-targeted patent ductus arteriosus (PDA) management strategy in preterm infants using the EL-Khuffash PDA Severity Score (PDAsc) for risk stratification. The objective was to compare outcomes between high- and low-risk infants from an early-targeted treatment epoch and a historical reference epoch who were risk stratified but did not undergo treatment.</p><p><strong>Methods: </strong>We conducted a single-centre, observational cohort study in a level III neonatal intensive care unit. Infants born <29 weeks gestation were stratified into high- and low-risk groups using the PDAsc. High-risk infants in the early-targeted treatment epoch received medical intervention, while low-risk infants did not. Outcomes from this epoch were compared with a historical reference epoch in which risk was assigned but treatment was not implemented. The primary outcomes included chronic lung disease (CLD), ventilation days and oxygen days.</p><p><strong>Results: </strong>A total of 110 high-risk and 74 low-risk infants were identified in the early-targeted epoch, compared with 84 high-risk and 51 low-risk infants in the reference epoch. High-risk infants in the early-targeted treatment epoch who achieved successful PDA closure demonstrated fewer ventilation days (median 5 vs 11), fewer oxygen days (median 45 vs 65) and a lower incidence of CLD (59% vs 76%) compared with high-risk infants in the reference epoch. However, high-risk infants in the early-targeted treatment epoch who failed treatment experienced outcomes similar to high-risk infants in the reference epoch. Low-risk infants in both epochs exhibited comparable favourable outcomes.</p><p><strong>Conclusions: </strong>The implementation of early-targeted risk-based PDA management may be associated with improved respiratory outcomes in high-risk infants who successfully responded to treatment. However, the observational nature of this study limits causal inferences. These findings underscore the need for further research, including randomised controlled trials with improved patient selection, to better understand the relationship between stratified treatment and important outcomes.</p>\",\"PeriodicalId\":9069,\"journal\":{\"name\":\"BMJ Paediatrics Open\",\"volume\":\"9 1\",\"pages\":\"\"},\"PeriodicalIF\":2.3000,\"publicationDate\":\"2025-07-16\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12273076/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"BMJ Paediatrics Open\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1136/bmjpo-2025-003347\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"PEDIATRICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMJ Paediatrics Open","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1136/bmjpo-2025-003347","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"PEDIATRICS","Score":null,"Total":0}
引用次数: 0
摘要
背景:本研究使用EL-Khuffash动脉导管未闭合严重程度评分(PDAsc)进行风险分层,评估早产儿早期靶向动脉导管未闭合(PDA)管理策略的结果。目的是比较来自早期靶向治疗时期和历史参考时期的高风险和低风险婴儿的结果,这些婴儿是危险分层的,但没有接受治疗。方法:我们在一个III级新生儿重症监护病房进行了一项单中心、观察队列研究。结果:在早期靶向期共发现110例高危婴儿和74例低危婴儿,而在参考期发现84例高危婴儿和51例低危婴儿。与参考时期的高危婴儿相比,在早期靶向治疗时期成功关闭PDA的高危婴儿通气天数更少(中位数5 vs 11),供氧天数更少(中位数45 vs 65), CLD发生率更低(59% vs 76%)。然而,在早期靶向治疗时期治疗失败的高危婴儿的结局与参考时期的高危婴儿相似。两个时期的低风险婴儿表现出相当有利的结果。结论:实施早期有针对性的基于风险的PDA管理可能与成功治疗的高危婴儿呼吸结局的改善有关。然而,这项研究的观察性质限制了因果推论。这些发现强调了进一步研究的必要性,包括改进患者选择的随机对照试验,以更好地了解分层治疗与重要结果之间的关系。
Does early-targeted risk-based management of a patent ductus arteriosus improve outcomes in preterm infants? Insights from an observational study.
Background: This study evaluates the outcomes of an early-targeted patent ductus arteriosus (PDA) management strategy in preterm infants using the EL-Khuffash PDA Severity Score (PDAsc) for risk stratification. The objective was to compare outcomes between high- and low-risk infants from an early-targeted treatment epoch and a historical reference epoch who were risk stratified but did not undergo treatment.
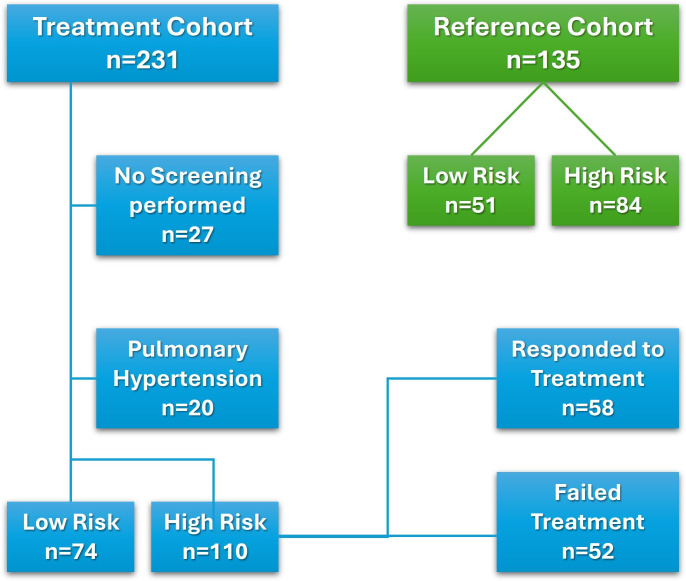
Methods: We conducted a single-centre, observational cohort study in a level III neonatal intensive care unit. Infants born <29 weeks gestation were stratified into high- and low-risk groups using the PDAsc. High-risk infants in the early-targeted treatment epoch received medical intervention, while low-risk infants did not. Outcomes from this epoch were compared with a historical reference epoch in which risk was assigned but treatment was not implemented. The primary outcomes included chronic lung disease (CLD), ventilation days and oxygen days.
Results: A total of 110 high-risk and 74 low-risk infants were identified in the early-targeted epoch, compared with 84 high-risk and 51 low-risk infants in the reference epoch. High-risk infants in the early-targeted treatment epoch who achieved successful PDA closure demonstrated fewer ventilation days (median 5 vs 11), fewer oxygen days (median 45 vs 65) and a lower incidence of CLD (59% vs 76%) compared with high-risk infants in the reference epoch. However, high-risk infants in the early-targeted treatment epoch who failed treatment experienced outcomes similar to high-risk infants in the reference epoch. Low-risk infants in both epochs exhibited comparable favourable outcomes.
Conclusions: The implementation of early-targeted risk-based PDA management may be associated with improved respiratory outcomes in high-risk infants who successfully responded to treatment. However, the observational nature of this study limits causal inferences. These findings underscore the need for further research, including randomised controlled trials with improved patient selection, to better understand the relationship between stratified treatment and important outcomes.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


