Mazda Farshad, Jana Felicitas Schader, Alexandra Stauffer, Carl Moritz Zipser, Najmeh Kheram, José Miguel Spirig, Marie-Rosa Fasser, Jonas Widmer, Vincent Hagel
{"title":"有无硬膜撕裂时膜间内窥镜下硬膜内、硬膜外和颅内压的变化。","authors":"Mazda Farshad, Jana Felicitas Schader, Alexandra Stauffer, Carl Moritz Zipser, Najmeh Kheram, José Miguel Spirig, Marie-Rosa Fasser, Jonas Widmer, Vincent Hagel","doi":"10.14245/ns.2550456.228","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>Endoscopic spine surgery implies possibly severe complications of the central nervous system, from headache to seizures and autonomic dysreflexia. These adverse events might be due to increased intracranial pressure (ICP), presumably induced by increased spinal intra-/epidural pressure caused by fluid irrigation. This study was designed to perform interlaminar endoscopic lumbar discectomy (IELD) at different irrigation fluid settings while monitoring its effect on intra-/epidural and ICPs, with and without dural tears.</p><p><strong>Methods: </strong>Spinal intradural pressures were measured by introducing catheters through a sacral approach to human cadavers' lumbar, thoracic, and cervical levels. Additionally, an epidural probe was placed at L3-4. ICP was measured by an intraventricular probe. IELD was performed at L3-4, and the effect of varying irrigation pressures by different endoscopic pump systems and gravity-based irrigation on intra-/epidural and ICP pressures was measured before and after durotomy at L3-4.</p><p><strong>Results: </strong>Intradural pressure at L3-4 correlated linearly with increasing irrigation pressure, irrespective of the used pump system (median pressure increase at 100-mmHg irrigation pressure: system I: 7 mmHg, r=0.94, p=0.002; system II: 7 mmHg, r=0.89, p=0.017) or gravity (8 mmHg, r=0.93, p=0.242). This effect was also seen intradurally at the thoracic/cervical spine, epidural, and intracranial level, and was even more pronounced with the maneuver of outflow-occlusion and a dural tear present.</p><p><strong>Conclusion: </strong>While performing IELD, pump pressures correlated linearly to intra-/epidural pressures and ICPs. Pressures did not rise to concerningly high levels without outflow-occlusion, even with increased pump pressures. In the presence of a dural tear, higher pump pressures exacerbated by occlusion may lead to deleterious intradural and ICP elevations.</p>","PeriodicalId":19269,"journal":{"name":"Neurospine","volume":"22 2","pages":"583-591"},"PeriodicalIF":3.6000,"publicationDate":"2025-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12242749/pdf/","citationCount":"0","resultStr":"{\"title\":\"Intra-, Epidural And Intracranial Pressure Changes During Interlaminar Endoscopy, With and Without Dural Tear.\",\"authors\":\"Mazda Farshad, Jana Felicitas Schader, Alexandra Stauffer, Carl Moritz Zipser, Najmeh Kheram, José Miguel Spirig, Marie-Rosa Fasser, Jonas Widmer, Vincent Hagel\",\"doi\":\"10.14245/ns.2550456.228\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>Endoscopic spine surgery implies possibly severe complications of the central nervous system, from headache to seizures and autonomic dysreflexia. These adverse events might be due to increased intracranial pressure (ICP), presumably induced by increased spinal intra-/epidural pressure caused by fluid irrigation. This study was designed to perform interlaminar endoscopic lumbar discectomy (IELD) at different irrigation fluid settings while monitoring its effect on intra-/epidural and ICPs, with and without dural tears.</p><p><strong>Methods: </strong>Spinal intradural pressures were measured by introducing catheters through a sacral approach to human cadavers' lumbar, thoracic, and cervical levels. Additionally, an epidural probe was placed at L3-4. ICP was measured by an intraventricular probe. IELD was performed at L3-4, and the effect of varying irrigation pressures by different endoscopic pump systems and gravity-based irrigation on intra-/epidural and ICP pressures was measured before and after durotomy at L3-4.</p><p><strong>Results: </strong>Intradural pressure at L3-4 correlated linearly with increasing irrigation pressure, irrespective of the used pump system (median pressure increase at 100-mmHg irrigation pressure: system I: 7 mmHg, r=0.94, p=0.002; system II: 7 mmHg, r=0.89, p=0.017) or gravity (8 mmHg, r=0.93, p=0.242). This effect was also seen intradurally at the thoracic/cervical spine, epidural, and intracranial level, and was even more pronounced with the maneuver of outflow-occlusion and a dural tear present.</p><p><strong>Conclusion: </strong>While performing IELD, pump pressures correlated linearly to intra-/epidural pressures and ICPs. Pressures did not rise to concerningly high levels without outflow-occlusion, even with increased pump pressures. In the presence of a dural tear, higher pump pressures exacerbated by occlusion may lead to deleterious intradural and ICP elevations.</p>\",\"PeriodicalId\":19269,\"journal\":{\"name\":\"Neurospine\",\"volume\":\"22 2\",\"pages\":\"583-591\"},\"PeriodicalIF\":3.6000,\"publicationDate\":\"2025-06-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12242749/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Neurospine\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.14245/ns.2550456.228\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/6/30 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q1\",\"JCRName\":\"CLINICAL NEUROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Neurospine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.14245/ns.2550456.228","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/6/30 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
Intra-, Epidural And Intracranial Pressure Changes During Interlaminar Endoscopy, With and Without Dural Tear.
Objective: Endoscopic spine surgery implies possibly severe complications of the central nervous system, from headache to seizures and autonomic dysreflexia. These adverse events might be due to increased intracranial pressure (ICP), presumably induced by increased spinal intra-/epidural pressure caused by fluid irrigation. This study was designed to perform interlaminar endoscopic lumbar discectomy (IELD) at different irrigation fluid settings while monitoring its effect on intra-/epidural and ICPs, with and without dural tears.
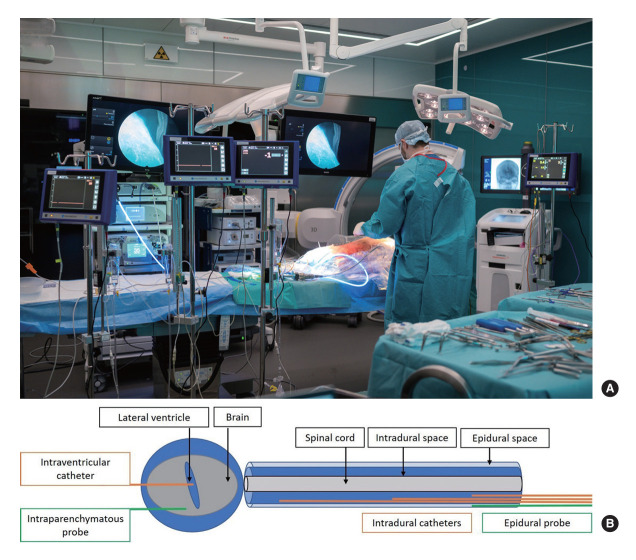
Methods: Spinal intradural pressures were measured by introducing catheters through a sacral approach to human cadavers' lumbar, thoracic, and cervical levels. Additionally, an epidural probe was placed at L3-4. ICP was measured by an intraventricular probe. IELD was performed at L3-4, and the effect of varying irrigation pressures by different endoscopic pump systems and gravity-based irrigation on intra-/epidural and ICP pressures was measured before and after durotomy at L3-4.
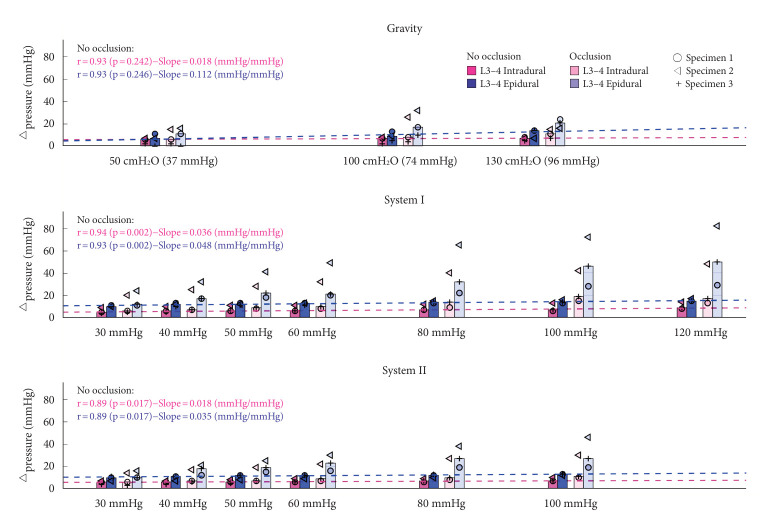
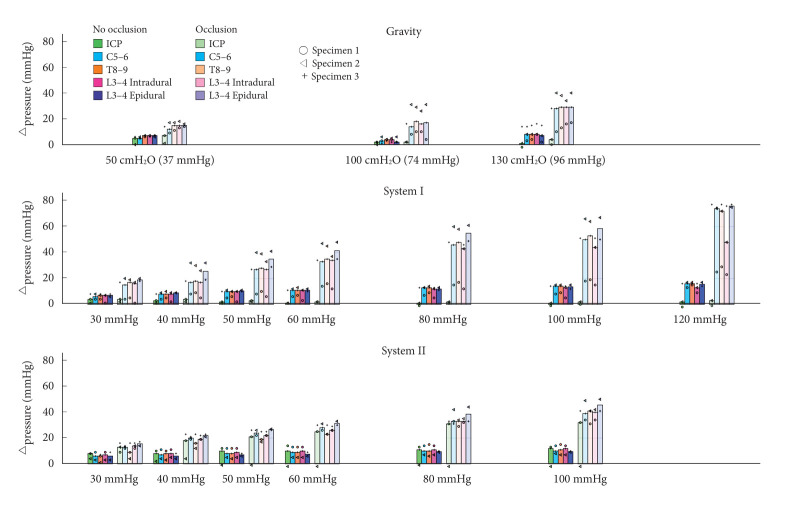
Results: Intradural pressure at L3-4 correlated linearly with increasing irrigation pressure, irrespective of the used pump system (median pressure increase at 100-mmHg irrigation pressure: system I: 7 mmHg, r=0.94, p=0.002; system II: 7 mmHg, r=0.89, p=0.017) or gravity (8 mmHg, r=0.93, p=0.242). This effect was also seen intradurally at the thoracic/cervical spine, epidural, and intracranial level, and was even more pronounced with the maneuver of outflow-occlusion and a dural tear present.
Conclusion: While performing IELD, pump pressures correlated linearly to intra-/epidural pressures and ICPs. Pressures did not rise to concerningly high levels without outflow-occlusion, even with increased pump pressures. In the presence of a dural tear, higher pump pressures exacerbated by occlusion may lead to deleterious intradural and ICP elevations.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


