{"title":"日本脑卒中外科学会会员对高血压脑出血手术干预设施的问卷调查。","authors":"Kazutaka Uchida, Shuntaro Kuwahara, Shoichiro Tsuji, Fumihiro Sakakibara, Manabu Shirakawa, Shinichi Yoshimura","doi":"10.2176/jns-nmc.2024-0340","DOIUrl":null,"url":null,"abstract":"<p><p>There is limited high-level evidence guiding the surgical treatment of hypertensive intracerebral hemorrhage, leaving the decision to the clinician's discretion. To understand treatment practices, a questionnaire survey was conducted among members of the Japanese Society on Surgery for Cerebral Stroke. This survey examined stroke care systems at various institutions, stroke numbers, and treatment details of patients with hypertensive intracerebral hemorrhage from January 2021 to December 2023. We examined data from 42 facilities, compared with 10 primary stroke centers cores and 32 non-primary stroke center cores. The total number of physicians involved in stroke care (primary stroke center cores vs. non-primary stroke center cores, median interquartile range; 18 [11-26] vs. 8 [4-14], p = 0.01), stroke specialists (8 [5-12] vs. 4 [2-7], p = 0.03), and supervising stroke surgeons (2 [1-2] vs. 1 [0-2], p = 0.008) was significantly higher in the primary stroke center cores group. Overall, 36,412 patients with stroke were hospitalized: 68% had cerebral infarction, 22% cerebral hemorrhage, 8% subarachnoid hemorrhage, and 2% other strokes. The locations of hypertensive intracerebral hemorrhage varied, with the putamen (31%), thalamus (25%), and lobe (24%) being predominantly affected. Non-invasive treatment was more prevalent in non-primary stroke center cores for most hypertensive intracerebral hemorrhage types, except for putaminal and brainstem hemorrhages. Surgical interventions were more common in primary stroke center cores, with craniotomies, neuroendoscopic surgeries, and ventricular drainage being preferred for cerebellar hemorrhage (28%), caudate nucleus hemorrhage (20%), and intraventricular hemorrhage (41%). This study highlights the treatment variability of hypertensive intracerebral hemorrhage between primary stroke center and non-primary stroke center cores.</p>","PeriodicalId":19225,"journal":{"name":"Neurologia medico-chirurgica","volume":" ","pages":"303-309"},"PeriodicalIF":2.3000,"publicationDate":"2025-07-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12322522/pdf/","citationCount":"0","resultStr":"{\"title\":\"Questionnaire Survey of Facilities Conducted among Members of the Japanese Society for Stroke Surgery on Surgical Intervention for Hypertensive Intracerebral Hemorrhage.\",\"authors\":\"Kazutaka Uchida, Shuntaro Kuwahara, Shoichiro Tsuji, Fumihiro Sakakibara, Manabu Shirakawa, Shinichi Yoshimura\",\"doi\":\"10.2176/jns-nmc.2024-0340\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>There is limited high-level evidence guiding the surgical treatment of hypertensive intracerebral hemorrhage, leaving the decision to the clinician's discretion. To understand treatment practices, a questionnaire survey was conducted among members of the Japanese Society on Surgery for Cerebral Stroke. This survey examined stroke care systems at various institutions, stroke numbers, and treatment details of patients with hypertensive intracerebral hemorrhage from January 2021 to December 2023. We examined data from 42 facilities, compared with 10 primary stroke centers cores and 32 non-primary stroke center cores. The total number of physicians involved in stroke care (primary stroke center cores vs. non-primary stroke center cores, median interquartile range; 18 [11-26] vs. 8 [4-14], p = 0.01), stroke specialists (8 [5-12] vs. 4 [2-7], p = 0.03), and supervising stroke surgeons (2 [1-2] vs. 1 [0-2], p = 0.008) was significantly higher in the primary stroke center cores group. Overall, 36,412 patients with stroke were hospitalized: 68% had cerebral infarction, 22% cerebral hemorrhage, 8% subarachnoid hemorrhage, and 2% other strokes. The locations of hypertensive intracerebral hemorrhage varied, with the putamen (31%), thalamus (25%), and lobe (24%) being predominantly affected. Non-invasive treatment was more prevalent in non-primary stroke center cores for most hypertensive intracerebral hemorrhage types, except for putaminal and brainstem hemorrhages. Surgical interventions were more common in primary stroke center cores, with craniotomies, neuroendoscopic surgeries, and ventricular drainage being preferred for cerebellar hemorrhage (28%), caudate nucleus hemorrhage (20%), and intraventricular hemorrhage (41%). This study highlights the treatment variability of hypertensive intracerebral hemorrhage between primary stroke center and non-primary stroke center cores.</p>\",\"PeriodicalId\":19225,\"journal\":{\"name\":\"Neurologia medico-chirurgica\",\"volume\":\" \",\"pages\":\"303-309\"},\"PeriodicalIF\":2.3000,\"publicationDate\":\"2025-07-15\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12322522/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Neurologia medico-chirurgica\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.2176/jns-nmc.2024-0340\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/5/29 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q2\",\"JCRName\":\"CLINICAL NEUROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Neurologia medico-chirurgica","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.2176/jns-nmc.2024-0340","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/5/29 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
Questionnaire Survey of Facilities Conducted among Members of the Japanese Society for Stroke Surgery on Surgical Intervention for Hypertensive Intracerebral Hemorrhage.
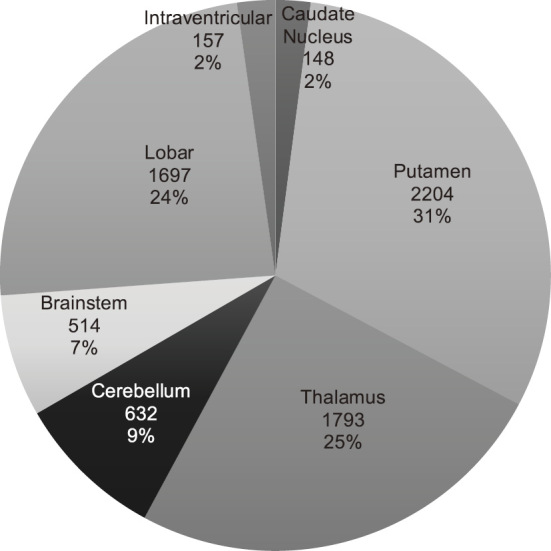
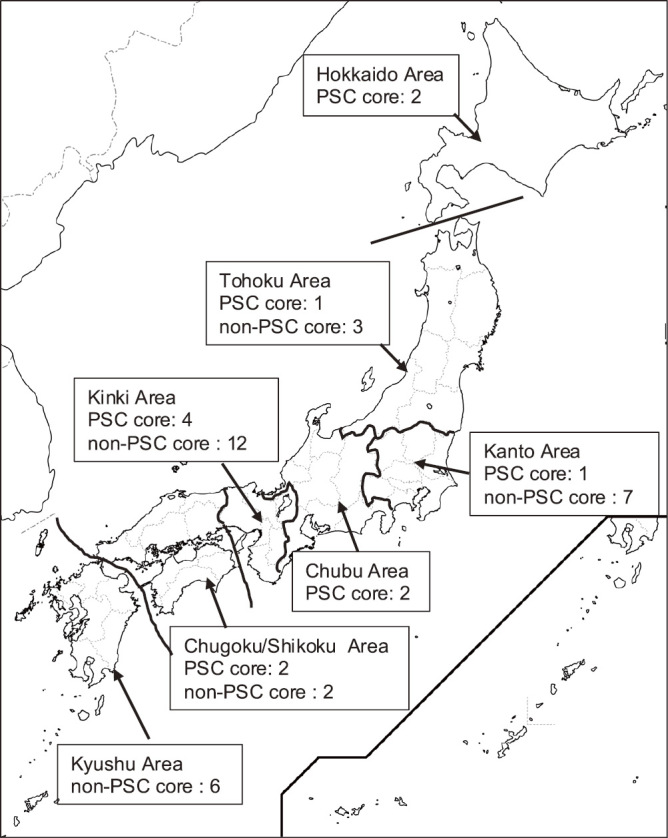
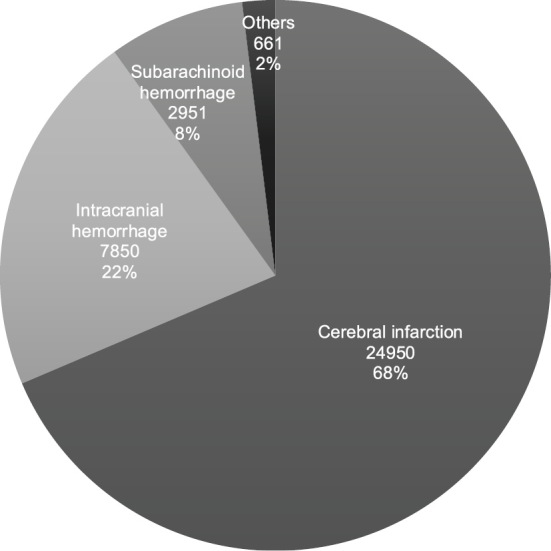
There is limited high-level evidence guiding the surgical treatment of hypertensive intracerebral hemorrhage, leaving the decision to the clinician's discretion. To understand treatment practices, a questionnaire survey was conducted among members of the Japanese Society on Surgery for Cerebral Stroke. This survey examined stroke care systems at various institutions, stroke numbers, and treatment details of patients with hypertensive intracerebral hemorrhage from January 2021 to December 2023. We examined data from 42 facilities, compared with 10 primary stroke centers cores and 32 non-primary stroke center cores. The total number of physicians involved in stroke care (primary stroke center cores vs. non-primary stroke center cores, median interquartile range; 18 [11-26] vs. 8 [4-14], p = 0.01), stroke specialists (8 [5-12] vs. 4 [2-7], p = 0.03), and supervising stroke surgeons (2 [1-2] vs. 1 [0-2], p = 0.008) was significantly higher in the primary stroke center cores group. Overall, 36,412 patients with stroke were hospitalized: 68% had cerebral infarction, 22% cerebral hemorrhage, 8% subarachnoid hemorrhage, and 2% other strokes. The locations of hypertensive intracerebral hemorrhage varied, with the putamen (31%), thalamus (25%), and lobe (24%) being predominantly affected. Non-invasive treatment was more prevalent in non-primary stroke center cores for most hypertensive intracerebral hemorrhage types, except for putaminal and brainstem hemorrhages. Surgical interventions were more common in primary stroke center cores, with craniotomies, neuroendoscopic surgeries, and ventricular drainage being preferred for cerebellar hemorrhage (28%), caudate nucleus hemorrhage (20%), and intraventricular hemorrhage (41%). This study highlights the treatment variability of hypertensive intracerebral hemorrhage between primary stroke center and non-primary stroke center cores.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


