Arafat A Farooqui, Syed M Mazhar Uddin, Sanjay K Maheshwari, Kevin Clements, Rabiah Ashraf, Jay Keith, Neha Sharma, Haris Bilal, Naira Saleem, Vijay S Shetty
{"title":"住院患者新发心房颤动。","authors":"Arafat A Farooqui, Syed M Mazhar Uddin, Sanjay K Maheshwari, Kevin Clements, Rabiah Ashraf, Jay Keith, Neha Sharma, Haris Bilal, Naira Saleem, Vijay S Shetty","doi":"10.55729/2000-9666.1467","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>To evaluate different factors precipitating new onset atrial fibrillation (AF) in hospitalized patients and their effect on in-patient mortality.</p><p><strong>Design: </strong>Retrospective cross-sectional study.</p><p><strong>Setting: </strong>Urban tertiary care center in New York City.</p><p><strong>Measurements: </strong>Primary outcomes:Determine different factors precipitating new onset atrial fibrillation in hospitalized patients and their effect on in-patient mortality.Secondary outcomes:Determine the duration of hospital stay after admission precipitating new onset atrial fibrillation and its effect on mortality.Evaluate different factors in COVID-19 patients with new onset atrial fibrillation.</p><p><strong>Results: </strong>Out of 464 patients; 62.3 % were males and 37.72 % were females. Evaluation of patients before developing new onset AF showed that 75.86 % had hypertension, 41.38 % had heart failure and 42.67 % had ischemic heart disease (IHD). Younger patients were noted to be treated with more rhythm control as compared to rate control (52.38 % vs 38.1 %) for their management while opposite was observed with patients >50 years of age (70.88 % vs 52.6 %; rate control vs rhythm control respectively). In terms of mortality, female gender (<i>OR</i> = 2.63, 95 % CI: 1.03-6.94, <i>p</i> = 0.045), presence of infection (<i>OR</i> = 6.00, 95 % CI: 2.23-18.08, <i>p</i> <0.001), use of vasopressors (<i>OR</i> = 6.71, 95 % CI: 2.58-19.42, <i>p</i>< 0.001), and a history of CVA (<i>OR</i> = 6.98, 95 % CI: 1.99-24.58, <i>p</i> = 0.002) all significantly increased the odds for mortality. Majority of the patients; 54.31 %, developed new onset AF after the third day of admission but it did not increase the mortality (OR 0.93, 95 % CI 0.37-2.45, p = 0.884). Majority of the patients (67 %) had enlarged left atrium (>35 ml/m<sup>2</sup>). However, it was not associated with higher mortality (OR 0.53, 95 % CI 0.19-1.48, p = 0.223). Patients that were tested positive for COVID-19 were more likely to have sepsis (75 % vs 31.46 %, <i>p</i>< 0.001).</p><p><strong>Conclusion: </strong>This study finds that four factors i.e., female gender, presence of infection, use of vasopressors, and a history of CVA all precipitate new onset atrial fibrillation with resultant increase in mortality during the same admission. Study concludes that longer hospital stay of more than three days increases the likelihood of developing new onset atrial fibrillation without increasing the mortality. Study found that patients who were positive forCOVID-19 were more likely to have sepsis.</p>","PeriodicalId":15460,"journal":{"name":"Journal of Community Hospital Internal Medicine Perspectives","volume":"15 2","pages":"25-32"},"PeriodicalIF":0.6000,"publicationDate":"2025-03-07","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12039332/pdf/","citationCount":"0","resultStr":"{\"title\":\"New Onset Atrial Fibrillation in Hospitalized Patients.\",\"authors\":\"Arafat A Farooqui, Syed M Mazhar Uddin, Sanjay K Maheshwari, Kevin Clements, Rabiah Ashraf, Jay Keith, Neha Sharma, Haris Bilal, Naira Saleem, Vijay S Shetty\",\"doi\":\"10.55729/2000-9666.1467\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objectives: </strong>To evaluate different factors precipitating new onset atrial fibrillation (AF) in hospitalized patients and their effect on in-patient mortality.</p><p><strong>Design: </strong>Retrospective cross-sectional study.</p><p><strong>Setting: </strong>Urban tertiary care center in New York City.</p><p><strong>Measurements: </strong>Primary outcomes:Determine different factors precipitating new onset atrial fibrillation in hospitalized patients and their effect on in-patient mortality.Secondary outcomes:Determine the duration of hospital stay after admission precipitating new onset atrial fibrillation and its effect on mortality.Evaluate different factors in COVID-19 patients with new onset atrial fibrillation.</p><p><strong>Results: </strong>Out of 464 patients; 62.3 % were males and 37.72 % were females. Evaluation of patients before developing new onset AF showed that 75.86 % had hypertension, 41.38 % had heart failure and 42.67 % had ischemic heart disease (IHD). Younger patients were noted to be treated with more rhythm control as compared to rate control (52.38 % vs 38.1 %) for their management while opposite was observed with patients >50 years of age (70.88 % vs 52.6 %; rate control vs rhythm control respectively). In terms of mortality, female gender (<i>OR</i> = 2.63, 95 % CI: 1.03-6.94, <i>p</i> = 0.045), presence of infection (<i>OR</i> = 6.00, 95 % CI: 2.23-18.08, <i>p</i> <0.001), use of vasopressors (<i>OR</i> = 6.71, 95 % CI: 2.58-19.42, <i>p</i>< 0.001), and a history of CVA (<i>OR</i> = 6.98, 95 % CI: 1.99-24.58, <i>p</i> = 0.002) all significantly increased the odds for mortality. Majority of the patients; 54.31 %, developed new onset AF after the third day of admission but it did not increase the mortality (OR 0.93, 95 % CI 0.37-2.45, p = 0.884). Majority of the patients (67 %) had enlarged left atrium (>35 ml/m<sup>2</sup>). However, it was not associated with higher mortality (OR 0.53, 95 % CI 0.19-1.48, p = 0.223). Patients that were tested positive for COVID-19 were more likely to have sepsis (75 % vs 31.46 %, <i>p</i>< 0.001).</p><p><strong>Conclusion: </strong>This study finds that four factors i.e., female gender, presence of infection, use of vasopressors, and a history of CVA all precipitate new onset atrial fibrillation with resultant increase in mortality during the same admission. Study concludes that longer hospital stay of more than three days increases the likelihood of developing new onset atrial fibrillation without increasing the mortality. Study found that patients who were positive forCOVID-19 were more likely to have sepsis.</p>\",\"PeriodicalId\":15460,\"journal\":{\"name\":\"Journal of Community Hospital Internal Medicine Perspectives\",\"volume\":\"15 2\",\"pages\":\"25-32\"},\"PeriodicalIF\":0.6000,\"publicationDate\":\"2025-03-07\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12039332/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Community Hospital Internal Medicine Perspectives\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.55729/2000-9666.1467\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"MEDICINE, GENERAL & INTERNAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Community Hospital Internal Medicine Perspectives","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.55729/2000-9666.1467","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
摘要
目的:探讨诱发住院患者新发房颤(AF)的不同因素及其对住院死亡率的影响。设计:回顾性横断面研究。地点:纽约市的城市三级保健中心。测量:主要结局:确定导致住院患者新发房颤的不同因素及其对住院患者死亡率的影响。次要结局:确定入院后新发房颤的住院时间及其对死亡率的影响。评价不同因素对新发房颤的影响。结果:464例患者中;男性占62.3%,女性占37.72%。对新发房颤患者的评估显示,75.86%的患者有高血压,41.38%的患者有心力衰竭,42.67%的患者有缺血性心脏病(IHD)。与率控制相比,年轻患者在治疗中注意到更多的节律控制(52.38%对38.1%),而在50岁以下的患者中观察到相反的情况(70.88%对52.6%;速率控制和节奏控制)。在死亡率方面,女性(OR = 2.63, 95% CI: 1.03-6.94, p = 0.045)、感染(OR = 6.00, 95% CI: 2.23-18.08, p OR = 6.71, 95% CI: 2.58-19.42, p< 0.001)和CVA病史(OR = 6.98, 95% CI: 1.99-24.58, p = 0.002)均显著增加了死亡率。大多数患者;54.31%的患者在入院第3天发生新发房源性心绞痛,但未增加死亡率(OR 0.93, 95% CI 0.37-2.45, p = 0.884)。大多数患者(67%)左心房增大(>35 ml/m2)。然而,它与较高的死亡率无关(OR 0.53, 95% CI 0.19-1.48, p = 0.223)。COVID-19检测呈阳性的患者更容易发生败血症(75%对31.46%,p< 0.001)。结论:本研究发现,女性、感染、使用血管加压药物和CVA史等四个因素都是新发房颤的诱因,导致同一次住院期间房颤死亡率增加。研究结论:住院时间超过3天会增加新发房颤的可能性,但不会增加死亡率。研究发现,covid -19阳性的患者更容易患败血症。
New Onset Atrial Fibrillation in Hospitalized Patients.
Objectives: To evaluate different factors precipitating new onset atrial fibrillation (AF) in hospitalized patients and their effect on in-patient mortality.
Design: Retrospective cross-sectional study.
Setting: Urban tertiary care center in New York City.
Measurements: Primary outcomes:Determine different factors precipitating new onset atrial fibrillation in hospitalized patients and their effect on in-patient mortality.Secondary outcomes:Determine the duration of hospital stay after admission precipitating new onset atrial fibrillation and its effect on mortality.Evaluate different factors in COVID-19 patients with new onset atrial fibrillation.
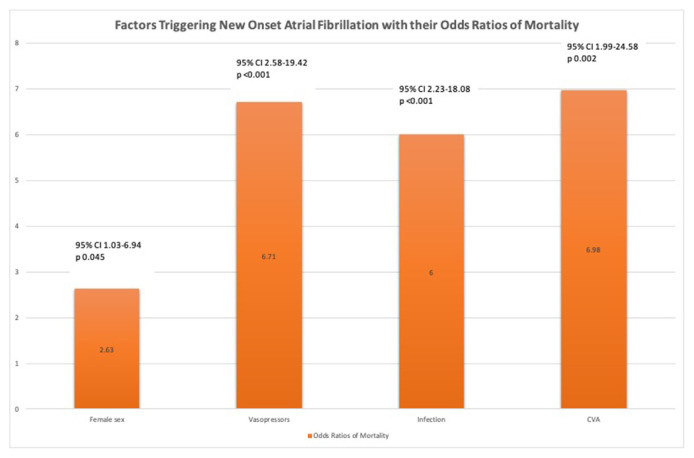
Results: Out of 464 patients; 62.3 % were males and 37.72 % were females. Evaluation of patients before developing new onset AF showed that 75.86 % had hypertension, 41.38 % had heart failure and 42.67 % had ischemic heart disease (IHD). Younger patients were noted to be treated with more rhythm control as compared to rate control (52.38 % vs 38.1 %) for their management while opposite was observed with patients >50 years of age (70.88 % vs 52.6 %; rate control vs rhythm control respectively). In terms of mortality, female gender (OR = 2.63, 95 % CI: 1.03-6.94, p = 0.045), presence of infection (OR = 6.00, 95 % CI: 2.23-18.08, p <0.001), use of vasopressors (OR = 6.71, 95 % CI: 2.58-19.42, p< 0.001), and a history of CVA (OR = 6.98, 95 % CI: 1.99-24.58, p = 0.002) all significantly increased the odds for mortality. Majority of the patients; 54.31 %, developed new onset AF after the third day of admission but it did not increase the mortality (OR 0.93, 95 % CI 0.37-2.45, p = 0.884). Majority of the patients (67 %) had enlarged left atrium (>35 ml/m2). However, it was not associated with higher mortality (OR 0.53, 95 % CI 0.19-1.48, p = 0.223). Patients that were tested positive for COVID-19 were more likely to have sepsis (75 % vs 31.46 %, p< 0.001).
Conclusion: This study finds that four factors i.e., female gender, presence of infection, use of vasopressors, and a history of CVA all precipitate new onset atrial fibrillation with resultant increase in mortality during the same admission. Study concludes that longer hospital stay of more than three days increases the likelihood of developing new onset atrial fibrillation without increasing the mortality. Study found that patients who were positive forCOVID-19 were more likely to have sepsis.
期刊介绍:
JCHIMP provides: up-to-date information in the field of Internal Medicine to community hospital medical professionals a platform for clinical faculty, residents, and medical students to publish research relevant to community hospital programs. Manuscripts that explore aspects of medicine at community hospitals welcome, including but not limited to: the best practices of community academic programs community hospital-based research opinion and insight from community hospital leadership and faculty the scholarly work of residents and medical students affiliated with community hospitals.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


