Qinguo Huang, Junhua Ye, Yanyu Wu, Qiang Zhou, Hong Li, Lin Peng, Yuntao Lu
{"title":"根据寰枕关节形态类型对伴有或不伴有II型颅底内陷的Chiari畸形的手术策略分析:对212例患者的回顾性研究。","authors":"Qinguo Huang, Junhua Ye, Yanyu Wu, Qiang Zhou, Hong Li, Lin Peng, Yuntao Lu","doi":"10.14245/ns.2449314.657","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>Our previous study categorized atlanto-occipital joint (AOJ) morphology into 3 types, with types II and III-AOJ associated with Chiari malformation (CM) with and without type II basilar invagination (II-BI), respectively. This study aimed to assess the feasibility of tailoring surgical strategies for patients with CM based on AOJ morphological types.</p><p><strong>Methods: </strong>We retrospectively studied 212 CM patients who underwent foramen magnum decompression (FMD) or combined occipitocervical fusion (OCF). Patients were divided into 4 groups: (1) pure CM with II-AOJ who underwent FMD (CM-II-FMD); (2) pure CM with III-AOJ who underwent FMD+OCF (CM-III-OCF); (3) CM-III-FMD; and (4) CM+ II-BI with III-AOJ who underwent FMD+OCF (BI-III-OCF). Clinical data, including manifestations, imaging findings, surgical details, and neurological assessments, were analyzed at the final follow-up to assess surgical efficacy.</p><p><strong>Results: </strong>Patients in the BI-III-OCF, CM-III-OCF, and CM-II-FMD groups exhibited a significant improvement in clinical symptoms (pain, sensory disturbances, motor weakness, gait ataxia, and bladder and bowel dysfunction) compared to preoperative levels (p<0.05). Results from the Japanese Orthopaedic Association scale and Neck Disability Index indicated a significant reduction in the degree of neurological impairment within these groups (p<0.05). Furthermore, the Chicago Chiari Outcome Scale scores indicated superior surgical outcomes for patients in these groups. Imaging analyses demonstrated significant reductions in the syringomyelic segment, syringomyelia width, and tonsillar herniation distance among these patients (p<0.05). However, the CM-III-FMD group did not significantly improve in these areas (p>0.05). Postoperative complications occurred in 4.3% of FMD+OCF patients and 3.3% of FMD-only patients.</p><p><strong>Conclusion: </strong>AOJ morphological types can guide surgical treatment strategies for CM with or without II-BI. FMD alone is suitable for II-AOJ cases, whereas III-AOJ cases should be treated with FMD combined with OCF.</p>","PeriodicalId":19269,"journal":{"name":"Neurospine","volume":" ","pages":"500-513"},"PeriodicalIF":3.6000,"publicationDate":"2025-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12242739/pdf/","citationCount":"0","resultStr":"{\"title\":\"Surgical Strategy Analysis of Chiari Malformation With or Without Type II Basilar Invagination According to the Morphological Types of the Atlanto-Occipital Joint: A Retrospective Study of 212 Patients.\",\"authors\":\"Qinguo Huang, Junhua Ye, Yanyu Wu, Qiang Zhou, Hong Li, Lin Peng, Yuntao Lu\",\"doi\":\"10.14245/ns.2449314.657\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>Our previous study categorized atlanto-occipital joint (AOJ) morphology into 3 types, with types II and III-AOJ associated with Chiari malformation (CM) with and without type II basilar invagination (II-BI), respectively. This study aimed to assess the feasibility of tailoring surgical strategies for patients with CM based on AOJ morphological types.</p><p><strong>Methods: </strong>We retrospectively studied 212 CM patients who underwent foramen magnum decompression (FMD) or combined occipitocervical fusion (OCF). Patients were divided into 4 groups: (1) pure CM with II-AOJ who underwent FMD (CM-II-FMD); (2) pure CM with III-AOJ who underwent FMD+OCF (CM-III-OCF); (3) CM-III-FMD; and (4) CM+ II-BI with III-AOJ who underwent FMD+OCF (BI-III-OCF). Clinical data, including manifestations, imaging findings, surgical details, and neurological assessments, were analyzed at the final follow-up to assess surgical efficacy.</p><p><strong>Results: </strong>Patients in the BI-III-OCF, CM-III-OCF, and CM-II-FMD groups exhibited a significant improvement in clinical symptoms (pain, sensory disturbances, motor weakness, gait ataxia, and bladder and bowel dysfunction) compared to preoperative levels (p<0.05). Results from the Japanese Orthopaedic Association scale and Neck Disability Index indicated a significant reduction in the degree of neurological impairment within these groups (p<0.05). Furthermore, the Chicago Chiari Outcome Scale scores indicated superior surgical outcomes for patients in these groups. Imaging analyses demonstrated significant reductions in the syringomyelic segment, syringomyelia width, and tonsillar herniation distance among these patients (p<0.05). However, the CM-III-FMD group did not significantly improve in these areas (p>0.05). Postoperative complications occurred in 4.3% of FMD+OCF patients and 3.3% of FMD-only patients.</p><p><strong>Conclusion: </strong>AOJ morphological types can guide surgical treatment strategies for CM with or without II-BI. FMD alone is suitable for II-AOJ cases, whereas III-AOJ cases should be treated with FMD combined with OCF.</p>\",\"PeriodicalId\":19269,\"journal\":{\"name\":\"Neurospine\",\"volume\":\" \",\"pages\":\"500-513\"},\"PeriodicalIF\":3.6000,\"publicationDate\":\"2025-06-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12242739/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Neurospine\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.14245/ns.2449314.657\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/4/16 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q1\",\"JCRName\":\"CLINICAL NEUROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Neurospine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.14245/ns.2449314.657","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/4/16 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
摘要
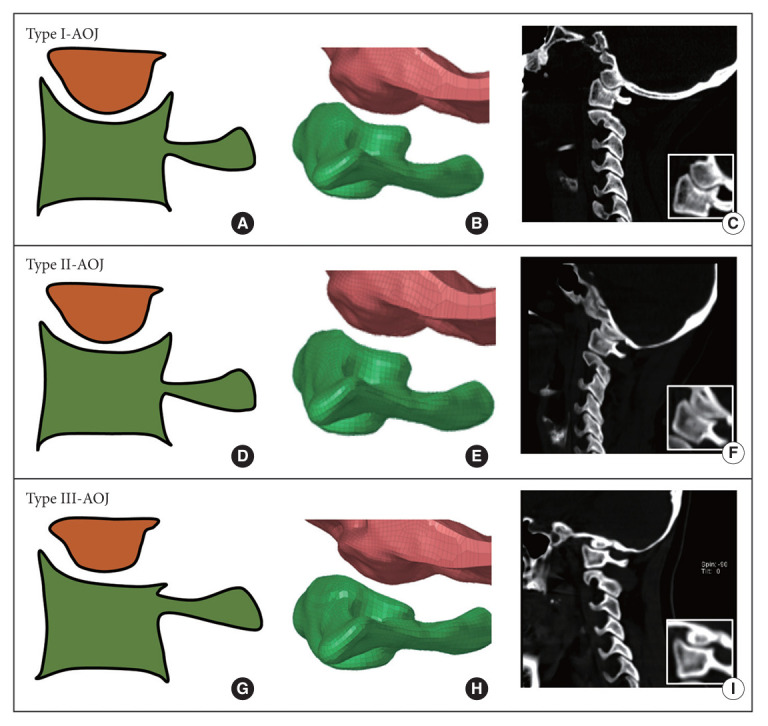
目的:我们之前的研究将寰枕关节(AOJ)形态分为三种类型,II型和III-AOJ分别与伴有和不伴有II型基底内陷(II- bi)的Chiari畸形(CM)相关。本研究旨在评估基于AOJ形态类型的CM患者定制手术策略的可行性。方法:我们回顾性研究了212例接受枕骨大孔减压(FMD)或枕颈融合(OCF)的CM患者。患者分为四组:(1)单纯CM合并II-AOJ行FMD (CM- ii -FMD);(2)单纯CM伴III-AOJ,行FMD + OCF者(CM- iii -OCF);(3) CM-III-FMD;(4) CM + II-BI伴III-AOJ行FMD + OCF者(BI-III-OCF)。在最后随访时分析临床资料,包括表现、影像学表现、手术细节和神经学评估,以评估手术疗效。结果:与术前相比,BI-III-OCF组、CM-III-OCF组和CM-II-FMD组患者的临床症状(疼痛、感觉障碍、运动无力、步态共济失调、膀胱和肠功能障碍)均有显著改善(p < 0.05)。日本骨科协会评分和颈部残疾指数结果显示,两组患者神经功能损伤程度均显著降低(p < 0.05)。此外,芝加哥Chiari预后量表评分显示,这两组患者的手术预后较好。影像学分析显示,这些患者的脊髓脊髓节段、脊髓脊髓宽度和扁桃体突出距离显著减少(p < 0.05)。而CM-III-FMD组在这些方面无明显改善(p < 0.05)。术后并发症发生率为FMD + OCF患者的4.3%,仅FMD患者的3.3%。结论:AOJ形态类型可指导伴有或不伴有II-BI的CM的手术治疗策略。手足口病单独适用于II-AOJ病例,而III-AOJ病例应联合手足口病治疗。
Surgical Strategy Analysis of Chiari Malformation With or Without Type II Basilar Invagination According to the Morphological Types of the Atlanto-Occipital Joint: A Retrospective Study of 212 Patients.
Objective: Our previous study categorized atlanto-occipital joint (AOJ) morphology into 3 types, with types II and III-AOJ associated with Chiari malformation (CM) with and without type II basilar invagination (II-BI), respectively. This study aimed to assess the feasibility of tailoring surgical strategies for patients with CM based on AOJ morphological types.
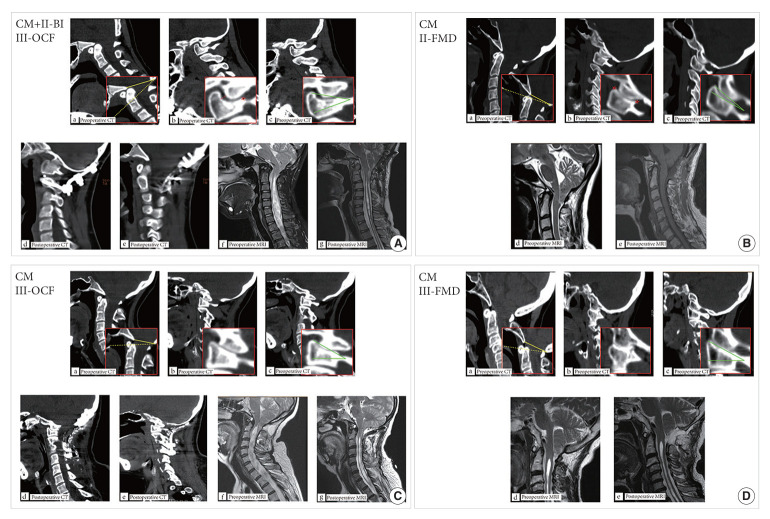
Methods: We retrospectively studied 212 CM patients who underwent foramen magnum decompression (FMD) or combined occipitocervical fusion (OCF). Patients were divided into 4 groups: (1) pure CM with II-AOJ who underwent FMD (CM-II-FMD); (2) pure CM with III-AOJ who underwent FMD+OCF (CM-III-OCF); (3) CM-III-FMD; and (4) CM+ II-BI with III-AOJ who underwent FMD+OCF (BI-III-OCF). Clinical data, including manifestations, imaging findings, surgical details, and neurological assessments, were analyzed at the final follow-up to assess surgical efficacy.
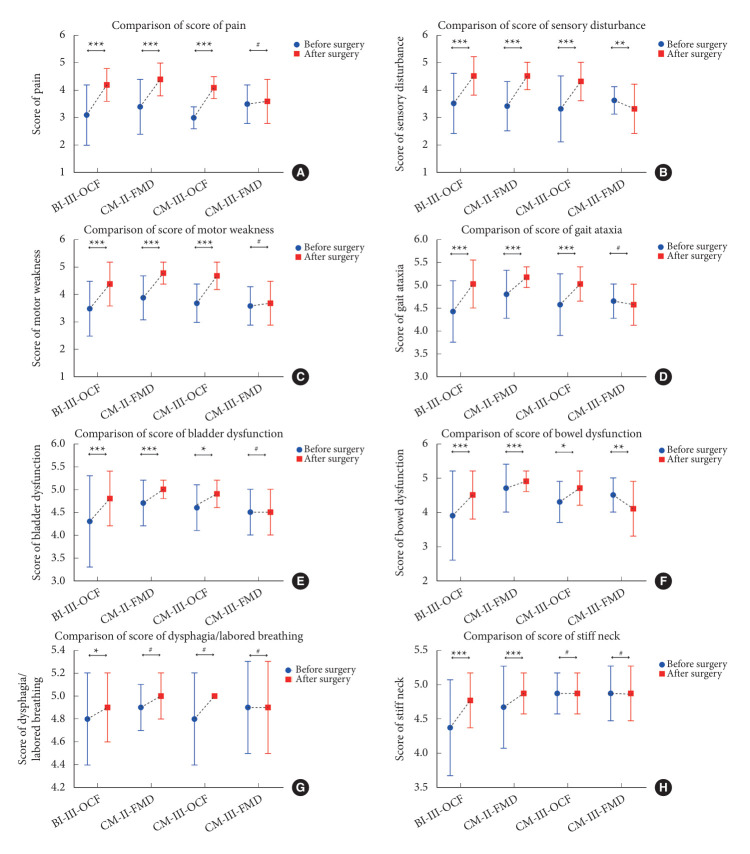
Results: Patients in the BI-III-OCF, CM-III-OCF, and CM-II-FMD groups exhibited a significant improvement in clinical symptoms (pain, sensory disturbances, motor weakness, gait ataxia, and bladder and bowel dysfunction) compared to preoperative levels (p<0.05). Results from the Japanese Orthopaedic Association scale and Neck Disability Index indicated a significant reduction in the degree of neurological impairment within these groups (p<0.05). Furthermore, the Chicago Chiari Outcome Scale scores indicated superior surgical outcomes for patients in these groups. Imaging analyses demonstrated significant reductions in the syringomyelic segment, syringomyelia width, and tonsillar herniation distance among these patients (p<0.05). However, the CM-III-FMD group did not significantly improve in these areas (p>0.05). Postoperative complications occurred in 4.3% of FMD+OCF patients and 3.3% of FMD-only patients.
Conclusion: AOJ morphological types can guide surgical treatment strategies for CM with or without II-BI. FMD alone is suitable for II-AOJ cases, whereas III-AOJ cases should be treated with FMD combined with OCF.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


