Sang Hun Lee, Micheal Raad, David B Cohen, Khaled M Kebaish, Lee H Riley Iii
{"title":"除了短钢板到椎间盘的距离外,“邻接水平骨化发展”的危险因素及其对邻接节段病理的临床意义。","authors":"Sang Hun Lee, Micheal Raad, David B Cohen, Khaled M Kebaish, Lee H Riley Iii","doi":"10.14245/ns.2448832.416","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>To identify factors associated with adjacent-level ossification development (ALOD) after anterior cervical discectomy and fusion (ACDF) and associated clinical outcomes.</p><p><strong>Methods: </strong>We retrospectively reviewed records of 140 adults who underwent primary ACDF for degenerative disc disease. We compared patients with and without ALOD after ACDF. Radiographic measurements and factors associated with ALOD were assessed preoperatively and at minimum 24-month follow-up. Clinical outcomes were incidence of clinical adjacent-segment pathologies (CASP), revision surgery, and patient-reported outcomes.</p><p><strong>Results: </strong>Factors associated with both cranial and caudal ALOD were short plate-to-disc distance (PDD), adjacent-segment kyphosis, hyperlordotic ACDF causing junctional segment kyphosis, and preoperative ossification of the anterior longitudinal ligament (OALL). Mean final adjacent-segment range of motion (ROM) was less in those with cranial ALOD (6.9° ± 2.8°) than in those without cranial ALOD (12° ± 4.2°) (p < 0.01). Mean final adjacent-segment ROM was also less in those with caudal ALOD (5.5° ± 2.4º) than in those without caudal ALOD (8.2º ± 3.7º) (p < 0.01). The incidence of CASP-required surgery was higher in those with caudal ALOD (p = 0.02) but no different in those with cranial ALOD (p = 0.69) compared with those without ALOD.</p><p><strong>Conclusion: </strong>Factors associated with ALOD were a kyphotic segment adjacent to ACDF, hyperlordotic fusion, preoperative OALL, and short PDD. ALOD was associated with less segmental ROM and, for those with caudal but not cranial ALOD, higher incidence of revision surgery for CASP.</p>","PeriodicalId":19269,"journal":{"name":"Neurospine","volume":"22 1","pages":"194-201"},"PeriodicalIF":3.6000,"publicationDate":"2025-03-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12010857/pdf/","citationCount":"0","resultStr":"{\"title\":\"Risk Factors for \\\"Adjacent-Level Ossification Development\\\" Other Than Short Plate-to-Disc Distance and Clinical Implications for Adjacent-Segment Pathology.\",\"authors\":\"Sang Hun Lee, Micheal Raad, David B Cohen, Khaled M Kebaish, Lee H Riley Iii\",\"doi\":\"10.14245/ns.2448832.416\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Purpose: </strong>To identify factors associated with adjacent-level ossification development (ALOD) after anterior cervical discectomy and fusion (ACDF) and associated clinical outcomes.</p><p><strong>Methods: </strong>We retrospectively reviewed records of 140 adults who underwent primary ACDF for degenerative disc disease. We compared patients with and without ALOD after ACDF. Radiographic measurements and factors associated with ALOD were assessed preoperatively and at minimum 24-month follow-up. Clinical outcomes were incidence of clinical adjacent-segment pathologies (CASP), revision surgery, and patient-reported outcomes.</p><p><strong>Results: </strong>Factors associated with both cranial and caudal ALOD were short plate-to-disc distance (PDD), adjacent-segment kyphosis, hyperlordotic ACDF causing junctional segment kyphosis, and preoperative ossification of the anterior longitudinal ligament (OALL). Mean final adjacent-segment range of motion (ROM) was less in those with cranial ALOD (6.9° ± 2.8°) than in those without cranial ALOD (12° ± 4.2°) (p < 0.01). Mean final adjacent-segment ROM was also less in those with caudal ALOD (5.5° ± 2.4º) than in those without caudal ALOD (8.2º ± 3.7º) (p < 0.01). The incidence of CASP-required surgery was higher in those with caudal ALOD (p = 0.02) but no different in those with cranial ALOD (p = 0.69) compared with those without ALOD.</p><p><strong>Conclusion: </strong>Factors associated with ALOD were a kyphotic segment adjacent to ACDF, hyperlordotic fusion, preoperative OALL, and short PDD. ALOD was associated with less segmental ROM and, for those with caudal but not cranial ALOD, higher incidence of revision surgery for CASP.</p>\",\"PeriodicalId\":19269,\"journal\":{\"name\":\"Neurospine\",\"volume\":\"22 1\",\"pages\":\"194-201\"},\"PeriodicalIF\":3.6000,\"publicationDate\":\"2025-03-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12010857/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Neurospine\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.14245/ns.2448832.416\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/3/31 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q1\",\"JCRName\":\"CLINICAL NEUROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Neurospine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.14245/ns.2448832.416","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/3/31 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
Risk Factors for "Adjacent-Level Ossification Development" Other Than Short Plate-to-Disc Distance and Clinical Implications for Adjacent-Segment Pathology.
Purpose: To identify factors associated with adjacent-level ossification development (ALOD) after anterior cervical discectomy and fusion (ACDF) and associated clinical outcomes.
Methods: We retrospectively reviewed records of 140 adults who underwent primary ACDF for degenerative disc disease. We compared patients with and without ALOD after ACDF. Radiographic measurements and factors associated with ALOD were assessed preoperatively and at minimum 24-month follow-up. Clinical outcomes were incidence of clinical adjacent-segment pathologies (CASP), revision surgery, and patient-reported outcomes.
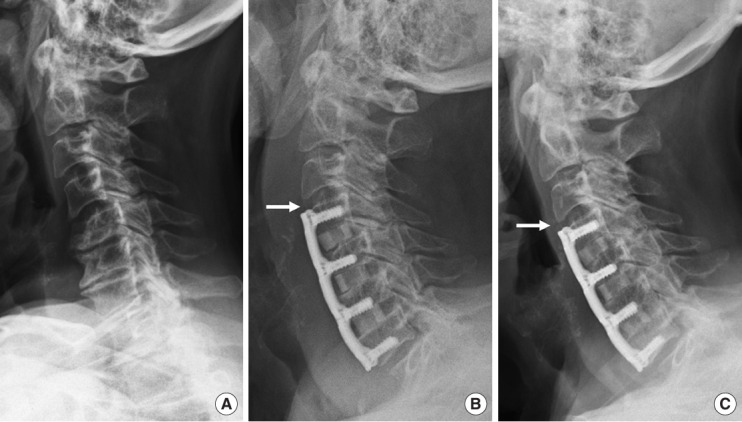
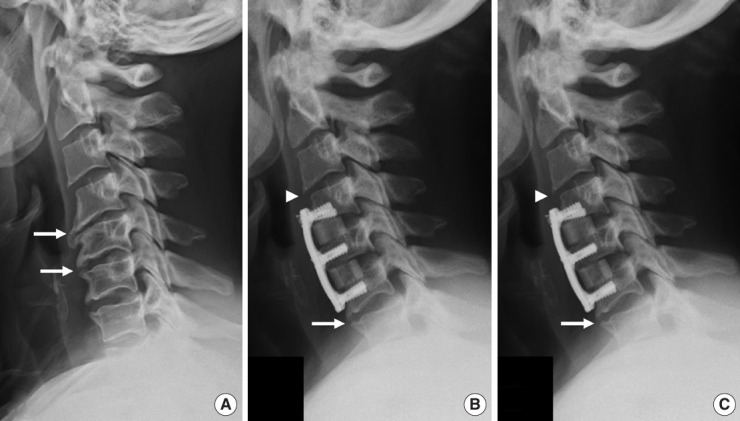
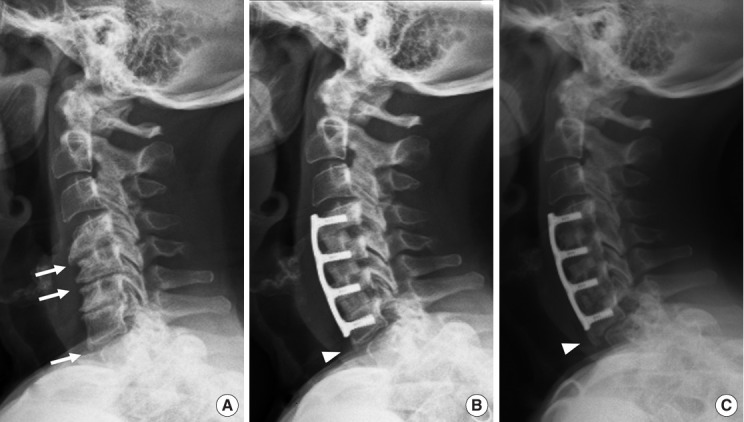
Results: Factors associated with both cranial and caudal ALOD were short plate-to-disc distance (PDD), adjacent-segment kyphosis, hyperlordotic ACDF causing junctional segment kyphosis, and preoperative ossification of the anterior longitudinal ligament (OALL). Mean final adjacent-segment range of motion (ROM) was less in those with cranial ALOD (6.9° ± 2.8°) than in those without cranial ALOD (12° ± 4.2°) (p < 0.01). Mean final adjacent-segment ROM was also less in those with caudal ALOD (5.5° ± 2.4º) than in those without caudal ALOD (8.2º ± 3.7º) (p < 0.01). The incidence of CASP-required surgery was higher in those with caudal ALOD (p = 0.02) but no different in those with cranial ALOD (p = 0.69) compared with those without ALOD.
Conclusion: Factors associated with ALOD were a kyphotic segment adjacent to ACDF, hyperlordotic fusion, preoperative OALL, and short PDD. ALOD was associated with less segmental ROM and, for those with caudal but not cranial ALOD, higher incidence of revision surgery for CASP.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


