{"title":"胸腰椎交界处骨质疏松性骨折球囊后凸成形术后邻近椎间盘高度与相邻椎体骨折发生的关系","authors":"Motonori Ishii, Yusuke Nishimura, Yu Yamamoto, Yoshitaka Nagashima, Takafumi Tanei, Masahito Hara, Masakazu Takayasu, Ryuta Saito","doi":"10.2176/jns-nmc.2024-0200","DOIUrl":null,"url":null,"abstract":"<p><p>Adjacent vertebral fractures after balloon kyphoplasty are speculated to occur in association with increased mechanical pressure due to rigid cement-augmented vertebrae. This study aimed to clarify whether adjacent vertebral fractures are more likely to occur after balloon kyphoplasty for osteoporotic vertebral fractures when the intervening adjacent disc degeneration is advanced. We retrospectively reviewed the findings for 99 patients who underwent balloon kyphoplasty for the first-ever osteoporotic vertebral fracture at the thoracolumbar junction levels (T11-L2). Radiological parameters and clinical data were compared for the cranial and caudal vertebrae between the groups with and without adjacent vertebral fractures within 1 year postoperatively. Postoperative adjacent vertebral fractures occurred in 20 patients (12 cranial adjacent vertebral fractures and eight caudal adjacent vertebral fractures). The cranial mean disc height was 5.87 ± 1.48 mm in the cranial adjacent vertebral fracture group and 7.98 ± 1.73 mm in the non-cranial adjacent vertebral fracture group (p < 0.01), and the caudal mean disc height was 6.24 ± 1.83 mm in the caudal adjacent vertebral fracture group and 9.55 ± 2.03 mm in the non-caudal adjacent vertebral fracture group (p < 0.01). According to receiver operating characteristic analysis, the optimized cutoff values of cranial mean disc height for cranial adjacent vertebral fracture occurrence and caudal mean disc height for caudal adjacent vertebral fracture occurrence were 6.37 mm and 7.70 mm, respectively. Multiple logistic regression models showed increased odds ratios for low disc height and large cement volume for cranial adjacent vertebral fractures and low disc height and cement leakage for caudal adjacent vertebral fractures. In conclusion, patients with advanced preoperative degeneration of the adjacent disc showed a higher incidence of adjacent vertebral fracture after balloon kyphoplasty.</p>","PeriodicalId":19225,"journal":{"name":"Neurologia medico-chirurgica","volume":" ","pages":"113-119"},"PeriodicalIF":2.3000,"publicationDate":"2025-03-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11968194/pdf/","citationCount":"0","resultStr":"{\"title\":\"Relationship between Preoperative Adjacent Disc Height and the Occurrence of Adjacent Vertebral Body Fractures after Balloon Kyphoplasty for Osteoporotic Fractures at the Thoracolumbar Junction.\",\"authors\":\"Motonori Ishii, Yusuke Nishimura, Yu Yamamoto, Yoshitaka Nagashima, Takafumi Tanei, Masahito Hara, Masakazu Takayasu, Ryuta Saito\",\"doi\":\"10.2176/jns-nmc.2024-0200\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Adjacent vertebral fractures after balloon kyphoplasty are speculated to occur in association with increased mechanical pressure due to rigid cement-augmented vertebrae. This study aimed to clarify whether adjacent vertebral fractures are more likely to occur after balloon kyphoplasty for osteoporotic vertebral fractures when the intervening adjacent disc degeneration is advanced. We retrospectively reviewed the findings for 99 patients who underwent balloon kyphoplasty for the first-ever osteoporotic vertebral fracture at the thoracolumbar junction levels (T11-L2). Radiological parameters and clinical data were compared for the cranial and caudal vertebrae between the groups with and without adjacent vertebral fractures within 1 year postoperatively. Postoperative adjacent vertebral fractures occurred in 20 patients (12 cranial adjacent vertebral fractures and eight caudal adjacent vertebral fractures). The cranial mean disc height was 5.87 ± 1.48 mm in the cranial adjacent vertebral fracture group and 7.98 ± 1.73 mm in the non-cranial adjacent vertebral fracture group (p < 0.01), and the caudal mean disc height was 6.24 ± 1.83 mm in the caudal adjacent vertebral fracture group and 9.55 ± 2.03 mm in the non-caudal adjacent vertebral fracture group (p < 0.01). According to receiver operating characteristic analysis, the optimized cutoff values of cranial mean disc height for cranial adjacent vertebral fracture occurrence and caudal mean disc height for caudal adjacent vertebral fracture occurrence were 6.37 mm and 7.70 mm, respectively. Multiple logistic regression models showed increased odds ratios for low disc height and large cement volume for cranial adjacent vertebral fractures and low disc height and cement leakage for caudal adjacent vertebral fractures. In conclusion, patients with advanced preoperative degeneration of the adjacent disc showed a higher incidence of adjacent vertebral fracture after balloon kyphoplasty.</p>\",\"PeriodicalId\":19225,\"journal\":{\"name\":\"Neurologia medico-chirurgica\",\"volume\":\" \",\"pages\":\"113-119\"},\"PeriodicalIF\":2.3000,\"publicationDate\":\"2025-03-15\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11968194/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Neurologia medico-chirurgica\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.2176/jns-nmc.2024-0200\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/2/10 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q2\",\"JCRName\":\"CLINICAL NEUROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Neurologia medico-chirurgica","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.2176/jns-nmc.2024-0200","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/2/10 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
摘要
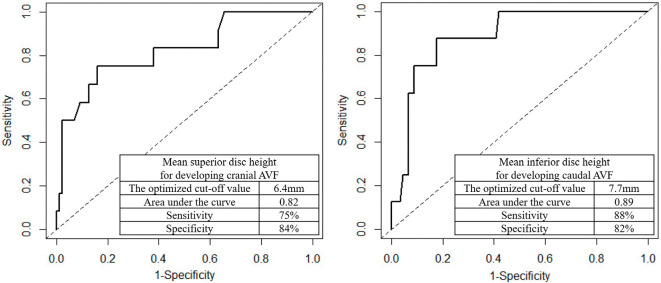
据推测,球囊后凸成形术后邻近椎体骨折的发生与刚性水泥增强椎体造成的机械压力增加有关。本研究旨在阐明当相邻椎间盘退变进展时,骨质疏松性椎体骨折球囊后凸成形术后是否更容易发生相邻椎体骨折。我们回顾性回顾了99例首次在胸腰段连接处(T11-L2)骨质疏松性椎体骨折接受球囊后凸成形术的患者的结果。比较术后1年内有无相邻椎体骨折组颅内和尾椎的影像学参数和临床资料。术后发生相邻椎体骨折20例(12例颅骨相邻椎体骨折,8例尾椎相邻椎体骨折)。颅侧邻近椎体骨折组的平均颅椎间盘高度为5.87±1.48 mm,非颅侧邻近椎体骨折组的平均颅椎间盘高度为7.98±1.73 mm (p < 0.01);尾侧邻近椎体骨折组的平均颅椎间盘高度为6.24±1.83 mm,非尾侧邻近椎体骨折组的平均颅椎间盘高度为9.55±2.03 mm (p < 0.01)。根据受试者工作特征分析,发生颅骨相邻椎体骨折的颅骨平均椎间盘高度和发生尾端相邻椎体骨折的尾端平均椎间盘高度的优化临界值分别为6.37 mm和7.70 mm。多元logistic回归模型显示,颅侧邻近椎体骨折的低椎间盘高度和大水泥体积的比值比增加,而尾侧邻近椎体骨折的低椎间盘高度和水泥泄漏的比值比增加。总之,术前临近椎间盘退变的患者在球囊后凸成形术后临近椎体骨折的发生率较高。
Relationship between Preoperative Adjacent Disc Height and the Occurrence of Adjacent Vertebral Body Fractures after Balloon Kyphoplasty for Osteoporotic Fractures at the Thoracolumbar Junction.
Adjacent vertebral fractures after balloon kyphoplasty are speculated to occur in association with increased mechanical pressure due to rigid cement-augmented vertebrae. This study aimed to clarify whether adjacent vertebral fractures are more likely to occur after balloon kyphoplasty for osteoporotic vertebral fractures when the intervening adjacent disc degeneration is advanced. We retrospectively reviewed the findings for 99 patients who underwent balloon kyphoplasty for the first-ever osteoporotic vertebral fracture at the thoracolumbar junction levels (T11-L2). Radiological parameters and clinical data were compared for the cranial and caudal vertebrae between the groups with and without adjacent vertebral fractures within 1 year postoperatively. Postoperative adjacent vertebral fractures occurred in 20 patients (12 cranial adjacent vertebral fractures and eight caudal adjacent vertebral fractures). The cranial mean disc height was 5.87 ± 1.48 mm in the cranial adjacent vertebral fracture group and 7.98 ± 1.73 mm in the non-cranial adjacent vertebral fracture group (p < 0.01), and the caudal mean disc height was 6.24 ± 1.83 mm in the caudal adjacent vertebral fracture group and 9.55 ± 2.03 mm in the non-caudal adjacent vertebral fracture group (p < 0.01). According to receiver operating characteristic analysis, the optimized cutoff values of cranial mean disc height for cranial adjacent vertebral fracture occurrence and caudal mean disc height for caudal adjacent vertebral fracture occurrence were 6.37 mm and 7.70 mm, respectively. Multiple logistic regression models showed increased odds ratios for low disc height and large cement volume for cranial adjacent vertebral fractures and low disc height and cement leakage for caudal adjacent vertebral fractures. In conclusion, patients with advanced preoperative degeneration of the adjacent disc showed a higher incidence of adjacent vertebral fracture after balloon kyphoplasty.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


