{"title":"类风湿性关节炎患者颈椎不稳定的相关因素:一项10年前瞻性多中心队列研究","authors":"Takashi Yurube, Yutaro Kanda, Hiroaki Hirata, Masatoshi Sumi","doi":"10.14245/ns.2448712.356","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>To identify factors associated with the absence of cervical spine instability in patients with rheumatoid arthritis (RA).</p><p><strong>Methods: </strong>Cervical spine instability was defined as the presence of at least one of the following: atlantoaxial subluxation, vertical subluxation of the axis, or subaxial subluxation. In 2001-2002, 634 enrolled outpatients with \"classical\" or \"definite\" RA underwent a radiographic cervical spine checkup. In 2012-2013, 233 (36.8%) prospectively underwent routine clinical follow-ups with a >10-year radiographic evaluation. The prevalence and independent predictive factors for no instability were analyzed by multivariable logistic regression. Next, 85 of 292 outpatients (29.1%) without baseline cervical spine instability completed consecutive >5-year and >10-year radiographic examinations. The incidence and predictors for no new development of instability were assessed similarly.</p><p><strong>Results: </strong>Among 233 patients, those without cervical spine instability decreased from 114 (48.9%) to 47 (20.2%) during >10 years. Steinbrocker peripheral joint destruction stages I-II (odds ratio [OR], 3.797; p=0.001), no corticosteroid administration (OR, 2.700; p=0.007), and no previous joint surgery (OR, 2.480; p=0.020) were predictors for no instability. Then, 33 of 85 (38.8%) consecutively followed patients without baseline cervical spine lesions did not develop instability throughout. Steinbrocker stages I-II (OR, 5.355; p=0.005) and no corticosteroid therapy (OR, 3.868; p=0.010) were predictors for no new onset of instability. C-reactive protein (CRP) level≤1.0 mg/dL was marginal in both models (n=233 [OR, 2.013; p=0.057], n=85 [OR, 2.453; p=0.075]).</p><p><strong>Conclusion: </strong>Steinbrocker stages I-II, no corticosteroids, no previous joint surgery, and possibly CRP ≤1.0 mg/dL are factors associated with >10-year absence of cervical spine instability in RA.</p>","PeriodicalId":19269,"journal":{"name":"Neurospine","volume":"21 4","pages":"1230-1240"},"PeriodicalIF":3.6000,"publicationDate":"2024-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11744530/pdf/","citationCount":"0","resultStr":"{\"title\":\"Factors Associated With the Absence of Cervical Spine Instability in Rheumatoid Arthritis: A >10-Year Prospective Multicenter Cohort Study.\",\"authors\":\"Takashi Yurube, Yutaro Kanda, Hiroaki Hirata, Masatoshi Sumi\",\"doi\":\"10.14245/ns.2448712.356\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>To identify factors associated with the absence of cervical spine instability in patients with rheumatoid arthritis (RA).</p><p><strong>Methods: </strong>Cervical spine instability was defined as the presence of at least one of the following: atlantoaxial subluxation, vertical subluxation of the axis, or subaxial subluxation. In 2001-2002, 634 enrolled outpatients with \\\"classical\\\" or \\\"definite\\\" RA underwent a radiographic cervical spine checkup. In 2012-2013, 233 (36.8%) prospectively underwent routine clinical follow-ups with a >10-year radiographic evaluation. The prevalence and independent predictive factors for no instability were analyzed by multivariable logistic regression. Next, 85 of 292 outpatients (29.1%) without baseline cervical spine instability completed consecutive >5-year and >10-year radiographic examinations. The incidence and predictors for no new development of instability were assessed similarly.</p><p><strong>Results: </strong>Among 233 patients, those without cervical spine instability decreased from 114 (48.9%) to 47 (20.2%) during >10 years. Steinbrocker peripheral joint destruction stages I-II (odds ratio [OR], 3.797; p=0.001), no corticosteroid administration (OR, 2.700; p=0.007), and no previous joint surgery (OR, 2.480; p=0.020) were predictors for no instability. Then, 33 of 85 (38.8%) consecutively followed patients without baseline cervical spine lesions did not develop instability throughout. Steinbrocker stages I-II (OR, 5.355; p=0.005) and no corticosteroid therapy (OR, 3.868; p=0.010) were predictors for no new onset of instability. C-reactive protein (CRP) level≤1.0 mg/dL was marginal in both models (n=233 [OR, 2.013; p=0.057], n=85 [OR, 2.453; p=0.075]).</p><p><strong>Conclusion: </strong>Steinbrocker stages I-II, no corticosteroids, no previous joint surgery, and possibly CRP ≤1.0 mg/dL are factors associated with >10-year absence of cervical spine instability in RA.</p>\",\"PeriodicalId\":19269,\"journal\":{\"name\":\"Neurospine\",\"volume\":\"21 4\",\"pages\":\"1230-1240\"},\"PeriodicalIF\":3.6000,\"publicationDate\":\"2024-12-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11744530/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Neurospine\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.14245/ns.2448712.356\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/12/31 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q1\",\"JCRName\":\"CLINICAL NEUROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Neurospine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.14245/ns.2448712.356","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/12/31 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
Factors Associated With the Absence of Cervical Spine Instability in Rheumatoid Arthritis: A >10-Year Prospective Multicenter Cohort Study.
Objective: To identify factors associated with the absence of cervical spine instability in patients with rheumatoid arthritis (RA).
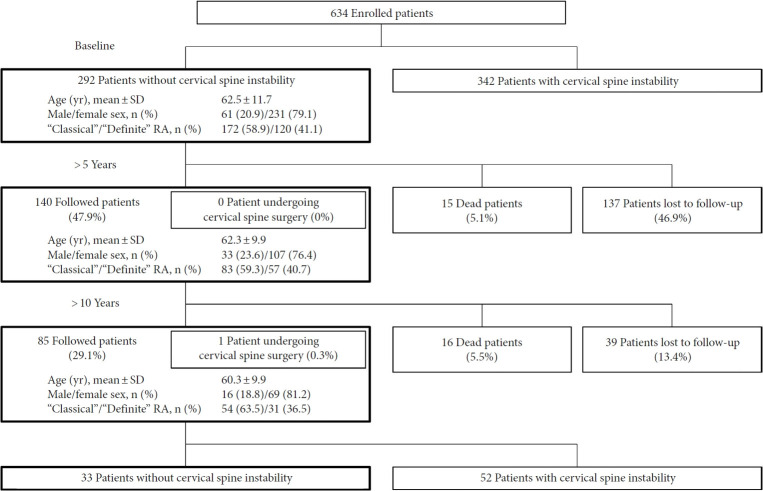
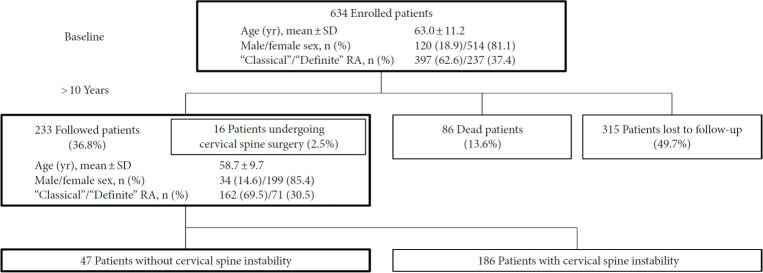
Methods: Cervical spine instability was defined as the presence of at least one of the following: atlantoaxial subluxation, vertical subluxation of the axis, or subaxial subluxation. In 2001-2002, 634 enrolled outpatients with "classical" or "definite" RA underwent a radiographic cervical spine checkup. In 2012-2013, 233 (36.8%) prospectively underwent routine clinical follow-ups with a >10-year radiographic evaluation. The prevalence and independent predictive factors for no instability were analyzed by multivariable logistic regression. Next, 85 of 292 outpatients (29.1%) without baseline cervical spine instability completed consecutive >5-year and >10-year radiographic examinations. The incidence and predictors for no new development of instability were assessed similarly.
Results: Among 233 patients, those without cervical spine instability decreased from 114 (48.9%) to 47 (20.2%) during >10 years. Steinbrocker peripheral joint destruction stages I-II (odds ratio [OR], 3.797; p=0.001), no corticosteroid administration (OR, 2.700; p=0.007), and no previous joint surgery (OR, 2.480; p=0.020) were predictors for no instability. Then, 33 of 85 (38.8%) consecutively followed patients without baseline cervical spine lesions did not develop instability throughout. Steinbrocker stages I-II (OR, 5.355; p=0.005) and no corticosteroid therapy (OR, 3.868; p=0.010) were predictors for no new onset of instability. C-reactive protein (CRP) level≤1.0 mg/dL was marginal in both models (n=233 [OR, 2.013; p=0.057], n=85 [OR, 2.453; p=0.075]).
Conclusion: Steinbrocker stages I-II, no corticosteroids, no previous joint surgery, and possibly CRP ≤1.0 mg/dL are factors associated with >10-year absence of cervical spine instability in RA.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


