{"title":"减少单门静脉全内窥镜腰椎椎体间融合术后神经系统并发症:GUARD技术联合延迟黄体韧带切除术的疗效。","authors":"Hao-Chun Chuang, Yu-Chia Hsu, Yuan-Fu Liu, Chao-Jui Chang, Yu-Meng Hsiao, Yi-Hung Huang, Keng-Chang Liu, Chien-Min Chen, Hyeun Sung Kim, Cheng-Li Lin","doi":"10.14245/ns.2448656.328","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>Uniportal full-endoscopic transforaminal lumbar interbody fusion (FE-TLIF) carries a unique risk of nerve traction and abrasion injury during cage insertion. This study aims to evaluate the clinical efficacy of the GUARD technique and delayed ligamentum flavectomy in reducing postoperative radicular pain and neurapraxia in patients undergoing uniportal FE-TLIF.</p><p><strong>Methods: </strong>A retrospective analysis was conducted on 45 patients with an average age of 53.9±12.4 years who underwent either FE facet-sparing TLIF (FE fs-TLIF) or FE facet-resecting TLIF (FE fr-TLIF). Patients were divided into 2 groups: the sentinel group (21 patients) using traditional sentinel pin techniques, and the GUARD group (24 patients) using the GUARD technique with delayed ligamentum flavectomy. Patient-reported outcomes included the visual analogue scale (VAS) for leg and back pain, and Oswestry Disability Index. Complication rates, including incidental durotomy, postoperative neurapraxia, and hematoma, were also documented.</p><p><strong>Results: </strong>Postoperative radicular pain in the legs was significantly reduced at 6 weeks in the GUARD group compared to the sentinel group (VAS: 2.201 vs. 3.267, p=0.021). The incidence of postoperative neurapraxia was markedly lower in the GUARD group (0% vs. 19%, p=0.047). Both groups showed similar improvements in disc height, segmental lordosis, and lumbar lordosis at the 1-year follow-up, with no significant differences in endplate injury or fusion rates.</p><p><strong>Conclusion: </strong>The GUARD technique and delayed ligamentum flavectomy significantly enhance patient safety by reducing postoperative radicular pain and neurapraxia without incurring additional costs. These techniques are easy to learn and integrate into existing surgical workflows, offering a valuable improvement for surgeons performing FE-TLIF procedures.</p>","PeriodicalId":19269,"journal":{"name":"Neurospine","volume":"21 4","pages":"1199-1209"},"PeriodicalIF":3.6000,"publicationDate":"2024-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11744540/pdf/","citationCount":"0","resultStr":"{\"title\":\"Reducing Postoperative Neurological Complications in Uniportal Full-Endoscopic Lumbar Interbody Fusion: Efficacy of the GUARD Technique Combined With Delayed Ligamentum Flavectomy.\",\"authors\":\"Hao-Chun Chuang, Yu-Chia Hsu, Yuan-Fu Liu, Chao-Jui Chang, Yu-Meng Hsiao, Yi-Hung Huang, Keng-Chang Liu, Chien-Min Chen, Hyeun Sung Kim, Cheng-Li Lin\",\"doi\":\"10.14245/ns.2448656.328\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>Uniportal full-endoscopic transforaminal lumbar interbody fusion (FE-TLIF) carries a unique risk of nerve traction and abrasion injury during cage insertion. This study aims to evaluate the clinical efficacy of the GUARD technique and delayed ligamentum flavectomy in reducing postoperative radicular pain and neurapraxia in patients undergoing uniportal FE-TLIF.</p><p><strong>Methods: </strong>A retrospective analysis was conducted on 45 patients with an average age of 53.9±12.4 years who underwent either FE facet-sparing TLIF (FE fs-TLIF) or FE facet-resecting TLIF (FE fr-TLIF). Patients were divided into 2 groups: the sentinel group (21 patients) using traditional sentinel pin techniques, and the GUARD group (24 patients) using the GUARD technique with delayed ligamentum flavectomy. Patient-reported outcomes included the visual analogue scale (VAS) for leg and back pain, and Oswestry Disability Index. Complication rates, including incidental durotomy, postoperative neurapraxia, and hematoma, were also documented.</p><p><strong>Results: </strong>Postoperative radicular pain in the legs was significantly reduced at 6 weeks in the GUARD group compared to the sentinel group (VAS: 2.201 vs. 3.267, p=0.021). The incidence of postoperative neurapraxia was markedly lower in the GUARD group (0% vs. 19%, p=0.047). Both groups showed similar improvements in disc height, segmental lordosis, and lumbar lordosis at the 1-year follow-up, with no significant differences in endplate injury or fusion rates.</p><p><strong>Conclusion: </strong>The GUARD technique and delayed ligamentum flavectomy significantly enhance patient safety by reducing postoperative radicular pain and neurapraxia without incurring additional costs. These techniques are easy to learn and integrate into existing surgical workflows, offering a valuable improvement for surgeons performing FE-TLIF procedures.</p>\",\"PeriodicalId\":19269,\"journal\":{\"name\":\"Neurospine\",\"volume\":\"21 4\",\"pages\":\"1199-1209\"},\"PeriodicalIF\":3.6000,\"publicationDate\":\"2024-12-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11744540/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Neurospine\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.14245/ns.2448656.328\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/12/31 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q1\",\"JCRName\":\"CLINICAL NEUROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Neurospine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.14245/ns.2448656.328","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/12/31 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
摘要
目的:单门静脉全内窥镜经椎间孔腰椎椎体间融合术(fe - tliff)有独特的风险,即在植入椎间孔时神经牵引和磨损损伤。本研究旨在评估GUARD技术和延迟黄韧带切除术在减轻单门FE-TLIF患者术后神经根痛和神经失用的临床疗效。方法:回顾性分析45例平均年龄53.9±12.4岁的患者,分别行保留FE面TLIF (FE fs-TLIF)和切除FE面TLIF (FE fr-TLIF)。将患者分为两组:哨兵组(21例)采用传统的前哨针技术,GUARD组(24例)采用GUARD技术联合延迟韧带黄体切除术。患者报告的结果包括腿部和背部疼痛的视觉模拟评分(VAS)和Oswestry残疾指数。并发症发生率,包括意外硬膜切开,术后神经失用和血肿,也被记录在案。结果:与前哨组相比,GUARD组术后6周时腿部神经根痛明显减轻(VAS: 2.201 vs. 3.267, p=0.021)。GUARD组术后神经失用发生率明显降低(0% vs. 19%, p=0.047)。在1年的随访中,两组在椎间盘高度、节段性前凸和腰椎前凸方面均有相似的改善,在终板损伤或融合率方面无显著差异。结论:GUARD技术和延迟黄韧带切除术通过减少术后神经根疼痛和神经失用显著提高患者的安全性,而不会产生额外的费用。这些技术易于学习并集成到现有的外科工作流程中,为外科医生进行FE-TLIF手术提供了有价值的改进。
Reducing Postoperative Neurological Complications in Uniportal Full-Endoscopic Lumbar Interbody Fusion: Efficacy of the GUARD Technique Combined With Delayed Ligamentum Flavectomy.
Objective: Uniportal full-endoscopic transforaminal lumbar interbody fusion (FE-TLIF) carries a unique risk of nerve traction and abrasion injury during cage insertion. This study aims to evaluate the clinical efficacy of the GUARD technique and delayed ligamentum flavectomy in reducing postoperative radicular pain and neurapraxia in patients undergoing uniportal FE-TLIF.
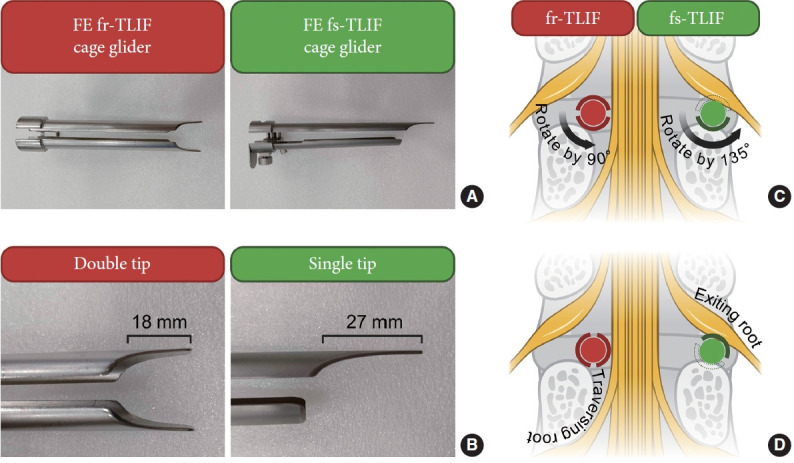
Methods: A retrospective analysis was conducted on 45 patients with an average age of 53.9±12.4 years who underwent either FE facet-sparing TLIF (FE fs-TLIF) or FE facet-resecting TLIF (FE fr-TLIF). Patients were divided into 2 groups: the sentinel group (21 patients) using traditional sentinel pin techniques, and the GUARD group (24 patients) using the GUARD technique with delayed ligamentum flavectomy. Patient-reported outcomes included the visual analogue scale (VAS) for leg and back pain, and Oswestry Disability Index. Complication rates, including incidental durotomy, postoperative neurapraxia, and hematoma, were also documented.
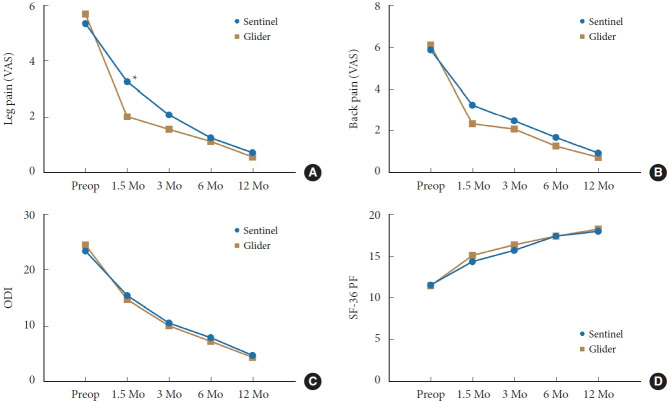
Results: Postoperative radicular pain in the legs was significantly reduced at 6 weeks in the GUARD group compared to the sentinel group (VAS: 2.201 vs. 3.267, p=0.021). The incidence of postoperative neurapraxia was markedly lower in the GUARD group (0% vs. 19%, p=0.047). Both groups showed similar improvements in disc height, segmental lordosis, and lumbar lordosis at the 1-year follow-up, with no significant differences in endplate injury or fusion rates.
Conclusion: The GUARD technique and delayed ligamentum flavectomy significantly enhance patient safety by reducing postoperative radicular pain and neurapraxia without incurring additional costs. These techniques are easy to learn and integrate into existing surgical workflows, offering a valuable improvement for surgeons performing FE-TLIF procedures.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


