George Athanasios Karpouzas, Bianca Papotti, Sarah R Ormseth, Marcella Palumbo, Elizabeth Hernandez, Maria Pia Adorni, Francesca Zimetti, Nicoletta Ronda
{"title":"血清胆固醇负荷能力的变化与类风湿关节炎患者冠状动脉粥样硬化的进展有关。","authors":"George Athanasios Karpouzas, Bianca Papotti, Sarah R Ormseth, Marcella Palumbo, Elizabeth Hernandez, Maria Pia Adorni, Francesca Zimetti, Nicoletta Ronda","doi":"10.1136/rmdopen-2024-004991","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>Excess cholesterol loading on arterial macrophages is linked to foam cell formation, atherosclerosis and cardiovascular risk in rheumatoid arthritis (RA). However, the effect of changes in cholesterol loading on coronary plaque trajectory and the impact of RA therapies on this relationship are unknown. We investigated the association between variations in cholesterol loading capacity (CLC) over time and atherosclerosis progression.</p><p><strong>Methods: </strong>In a prospective observational cohort study, coronary CT angiography evaluated atherosclerosis (non-calcified, partially calcified or fully calcified plaques and coronary artery calcium (CAC) score) in 100 patients with RA without cardiovascular disease at baseline and 6.9±0.4 years later. The presence of ≥5 plaques and lesions rendering >50% stenosis was considered an extensive and obstructive disease, respectively. Serum CLC was measured on human THP-1 monocyte-derived macrophages with a fluorometric assay.</p><p><strong>Results: </strong>Mean CLC change (follow-up CLC-baseline CLC) was 1.54 (SD 3.69) μg cholesterol/mg protein. In models adjusting for atherosclerotic cardiovascular disease risk score, baseline plaque and other relevant covariates, CLC change (per SD unit increase) is associated with a higher likelihood of progression of non-calcified (OR 2.55, 95% CI 1.22 to 5.35), fully calcified plaque (OR 3.10, 95% CI 1.67 to 5.76), CAC (OR 1.80, 95% CI 1.18 to 2.74) and new extensive or obstructive disease (OR 2.43, 95% CI 1.11 to 5.34). Exposure to prednisone unfavourably influenced, while biologics and statins favourably affected the relationship between CLC change and atherosclerosis progression (all p-for-interactions ≤0.048).</p><p><strong>Conclusion: </strong>CLC change is associated with atherosclerosis progression in a dose-dependent manner, including lipid-rich non-calcified plaques and extensive or obstructive disease that yield the greatest cardiovascular risk.</p>","PeriodicalId":21396,"journal":{"name":"RMD Open","volume":"10 4","pages":""},"PeriodicalIF":4.7000,"publicationDate":"2024-12-24","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11683967/pdf/","citationCount":"0","resultStr":"{\"title\":\"Changes in serum cholesterol loading capacity are linked to coronary atherosclerosis progression in rheumatoid arthritis.\",\"authors\":\"George Athanasios Karpouzas, Bianca Papotti, Sarah R Ormseth, Marcella Palumbo, Elizabeth Hernandez, Maria Pia Adorni, Francesca Zimetti, Nicoletta Ronda\",\"doi\":\"10.1136/rmdopen-2024-004991\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>Excess cholesterol loading on arterial macrophages is linked to foam cell formation, atherosclerosis and cardiovascular risk in rheumatoid arthritis (RA). However, the effect of changes in cholesterol loading on coronary plaque trajectory and the impact of RA therapies on this relationship are unknown. We investigated the association between variations in cholesterol loading capacity (CLC) over time and atherosclerosis progression.</p><p><strong>Methods: </strong>In a prospective observational cohort study, coronary CT angiography evaluated atherosclerosis (non-calcified, partially calcified or fully calcified plaques and coronary artery calcium (CAC) score) in 100 patients with RA without cardiovascular disease at baseline and 6.9±0.4 years later. The presence of ≥5 plaques and lesions rendering >50% stenosis was considered an extensive and obstructive disease, respectively. Serum CLC was measured on human THP-1 monocyte-derived macrophages with a fluorometric assay.</p><p><strong>Results: </strong>Mean CLC change (follow-up CLC-baseline CLC) was 1.54 (SD 3.69) μg cholesterol/mg protein. In models adjusting for atherosclerotic cardiovascular disease risk score, baseline plaque and other relevant covariates, CLC change (per SD unit increase) is associated with a higher likelihood of progression of non-calcified (OR 2.55, 95% CI 1.22 to 5.35), fully calcified plaque (OR 3.10, 95% CI 1.67 to 5.76), CAC (OR 1.80, 95% CI 1.18 to 2.74) and new extensive or obstructive disease (OR 2.43, 95% CI 1.11 to 5.34). Exposure to prednisone unfavourably influenced, while biologics and statins favourably affected the relationship between CLC change and atherosclerosis progression (all p-for-interactions ≤0.048).</p><p><strong>Conclusion: </strong>CLC change is associated with atherosclerosis progression in a dose-dependent manner, including lipid-rich non-calcified plaques and extensive or obstructive disease that yield the greatest cardiovascular risk.</p>\",\"PeriodicalId\":21396,\"journal\":{\"name\":\"RMD Open\",\"volume\":\"10 4\",\"pages\":\"\"},\"PeriodicalIF\":4.7000,\"publicationDate\":\"2024-12-24\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11683967/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"RMD Open\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1136/rmdopen-2024-004991\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"RHEUMATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"RMD Open","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1136/rmdopen-2024-004991","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"RHEUMATOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
目的:动脉巨噬细胞的过量胆固醇负荷与类风湿关节炎(RA)的泡沫细胞形成、动脉粥样硬化和心血管风险有关。然而,胆固醇负荷变化对冠状动脉斑块轨迹的影响以及类风湿性关节炎治疗对这种关系的影响尚不清楚。我们研究了胆固醇负荷能力(CLC)随时间变化与动脉粥样硬化进展之间的关系。方法:在一项前瞻性观察队列研究中,冠状动脉CT血管造影评估100例无心血管疾病的RA患者在基线和6.9±0.4年后的动脉粥样硬化(非钙化、部分钙化或完全钙化斑块和冠状动脉钙(CAC)评分)。≥5个斑块和50%狭窄的病变分别被认为是广泛和阻塞性疾病。用荧光法测定人THP-1单核细胞源性巨噬细胞的血清CLC。结果:平均CLC变化(随访CLC-基线CLC)为1.54 (SD 3.69) μg胆固醇/mg蛋白。在校正动脉粥样硬化性心血管疾病风险评分、基线斑块和其他相关变量的模型中,CLC变化(每SD单位增加)与非钙化(OR 2.55, 95% CI 1.22至5.35)、完全钙化斑块(OR 3.10, 95% CI 1.67至5.76)、CAC (OR 1.80, 95% CI 1.18至2.74)和新的广泛或阻塞性疾病(OR 2.43, 95% CI 1.11至5.34)进展的可能性较高相关。暴露于泼尼松不利影响,而生物制剂和他汀类药物有利影响CLC变化和动脉粥样硬化进展之间的关系(所有相互作用的p值≤0.048)。结论:CLC变化与动脉粥样硬化进展呈剂量依赖性,包括富含脂质的非钙化斑块和广泛或阻塞性疾病,这些疾病可产生最大的心血管风险。
Changes in serum cholesterol loading capacity are linked to coronary atherosclerosis progression in rheumatoid arthritis.
Objective: Excess cholesterol loading on arterial macrophages is linked to foam cell formation, atherosclerosis and cardiovascular risk in rheumatoid arthritis (RA). However, the effect of changes in cholesterol loading on coronary plaque trajectory and the impact of RA therapies on this relationship are unknown. We investigated the association between variations in cholesterol loading capacity (CLC) over time and atherosclerosis progression.
Methods: In a prospective observational cohort study, coronary CT angiography evaluated atherosclerosis (non-calcified, partially calcified or fully calcified plaques and coronary artery calcium (CAC) score) in 100 patients with RA without cardiovascular disease at baseline and 6.9±0.4 years later. The presence of ≥5 plaques and lesions rendering >50% stenosis was considered an extensive and obstructive disease, respectively. Serum CLC was measured on human THP-1 monocyte-derived macrophages with a fluorometric assay.
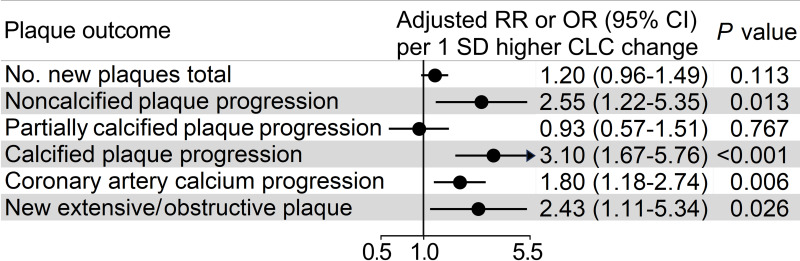
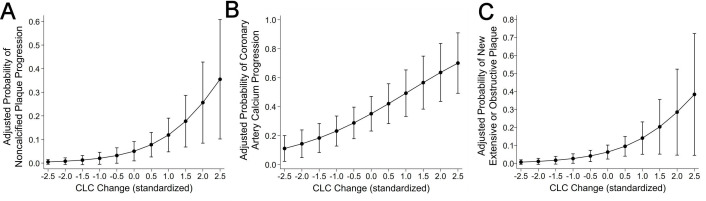
Results: Mean CLC change (follow-up CLC-baseline CLC) was 1.54 (SD 3.69) μg cholesterol/mg protein. In models adjusting for atherosclerotic cardiovascular disease risk score, baseline plaque and other relevant covariates, CLC change (per SD unit increase) is associated with a higher likelihood of progression of non-calcified (OR 2.55, 95% CI 1.22 to 5.35), fully calcified plaque (OR 3.10, 95% CI 1.67 to 5.76), CAC (OR 1.80, 95% CI 1.18 to 2.74) and new extensive or obstructive disease (OR 2.43, 95% CI 1.11 to 5.34). Exposure to prednisone unfavourably influenced, while biologics and statins favourably affected the relationship between CLC change and atherosclerosis progression (all p-for-interactions ≤0.048).
Conclusion: CLC change is associated with atherosclerosis progression in a dose-dependent manner, including lipid-rich non-calcified plaques and extensive or obstructive disease that yield the greatest cardiovascular risk.
期刊介绍:
RMD Open publishes high quality peer-reviewed original research covering the full spectrum of musculoskeletal disorders, rheumatism and connective tissue diseases, including osteoporosis, spine and rehabilitation. Clinical and epidemiological research, basic and translational medicine, interesting clinical cases, and smaller studies that add to the literature are all considered.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


