Monia Di Prete, Alessandra Latini, Viviana Lora, Fulvia Pimpinelli, Carlo Cota
{"title":"肉芽肿性继发性梅毒:何时保持高度怀疑?","authors":"Monia Di Prete, Alessandra Latini, Viviana Lora, Fulvia Pimpinelli, Carlo Cota","doi":"10.1111/cup.14702","DOIUrl":null,"url":null,"abstract":"<p>We recently read with great interest, the publication entitled “Granulomatous secondary syphilis: Another diagnostic pitfall for dermatopathologist” concerning a case of secondary syphilis with granulomatous inflammation on histopathology, which was immunohistochemically negative for <i>Treponema pallidum</i>.<span><sup>1</sup></span> Jin et al. underlined that granulomatous infiltration is uncommon in cases of secondary syphilis cutaneous lesions. In these cases, detecting the spirochetes may be difficult, as the number of microorganisms decreases in established, non-treated infections. Although the <i>T. pallidum</i> immunohistochemistry is highly sensitive and can detect even a small number of pathogens, the case described in the paper failed to stain. It was possible to establish the correct diagnosis by matching serological results.<span><sup>1</sup></span></p><p>Recently, a 48-year-old Caucasian woman visited our unit with a diffuse rash, which was present for 3 months without any other symptoms. The eruption consisted of widespread erythematous papules and nodules on the trunk and extremities without the involvement of the mucous membranes, palms, and soles (Figure 1A,B). She was referred to us by an external dermatologist with the suspected diagnosis of cutaneous lymphoma. The histopathological examination of a punch-biopsy specimen, a lesion on the left flank, revealed a granulomatous inflammatory infiltration in the dermis, with perivascular distribution (Figure 1C). At higher magnification, the epithelioid granulomas were surrounded by small lymphocytes and numerous plasma cells (Figure 1D). Immunohistochemistry for <i>T. pallidum</i> failed to reveal organisms. Despite the negativity of the stain, the histopathology was highly suspicious of secondary granulomatous syphilis; therefore, we suggested performing serological investigations to confirm the diagnosis of syphilis; both the Venereal Disease Research Laboratory and the <i>T. pallidum</i> hemagglutination assay (TPHA) were negative. The patient returned to us 3 weeks later due to the development of new lesions on the oral mucosa and a single lesion on the sole of the right foot. We decided to directly test for <i>T. pallidum</i> from an exudative lesion on the trunk using a real-time polymerase chain reaction (PCR) assay, which finally resulted in a positive detection. We repeated the serology in the Microbiology Laboratory of our Hospital on the same day of the cutaneous swab, and at this time, it resulted positive in syphilis, with a rapid plasma reagin (RPR) titer of 1:64 and a TPHA titer of 1:2560 and negative for HIV.</p><p>The patient received two intramuscular injections of 1 200 000 units of diaminocillin, preceded by 4 mg of betamethasone, resulting in complete remission of the disease.</p><p>Syphilis still represents a diagnostic pitfall for dermatologists and dermatopathologists, as it may manifest with a variety of clinical and histopathological features. From a clinical point-of-view, involvement of the palms and soles is typical of secondary syphilis. In cases of granulomatous syphilis, these sites are less commonly affected or may not be involved at all. Detecting the spirochetes using immunohistochemistry on the tissue samples may be challenging in these instances. The reason for this phenomenon is not clear, but it has been hypothesized that an impairment in the delayed-type hypersensitivity reaction, leading to chronic granulomatous inflammation, may be responsible.<span><sup>1</sup></span> In our case, the negativity for both treponemal and non-treponemal serological tests noticed the first time is explainable by the “hook effect” or “prozone phenomenon,” which is an immunological phenomenon whereby the immune complexes formation is impaired by the very high concentration of an antibody or an antigen, resulting in a false negative assay. This phenomenon has been reported in patients with HIV co-infection,<span><sup>2</sup></span> but it may occur also in patients with secondary syphilis characterized by a very high antibody titer.<span><sup>3</sup></span></p><p>Our case emphasizes the continued importance of conventional histology, based on hematoxylin–eosin in order to provide an accurate diagnosis. The presence of numerous plasma cells in the context of a granulomatous inflammation led us to be highly suspicious of secondary syphilis, even when both immunohistochemistry and serology were negative. In these cases, a PCR assay is helpful to confirm the diagnosis.<span><sup>4</sup></span> In fact, the negativity of the ancillary immunohistochemical techniques should not suggest the prompt exclusion of infectious diseases, especially in cases of granulomatous inflammation, when the microorganisms may be present in very small numbers. Moreover, serological tests may result in false negatives in some cases, therefore, RPR should be repeated with the diluted serum to reach a correct diagnosis and to avoid the “prozone phenomenon,” which contributes to misdiagnosis.</p>","PeriodicalId":15407,"journal":{"name":"Journal of Cutaneous Pathology","volume":"51 11","pages":"866-867"},"PeriodicalIF":1.6000,"publicationDate":"2024-08-14","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/cup.14702","citationCount":"0","resultStr":"{\"title\":\"Granulomatous secondary syphilis: When to maintain a high index of suspicion?\",\"authors\":\"Monia Di Prete, Alessandra Latini, Viviana Lora, Fulvia Pimpinelli, Carlo Cota\",\"doi\":\"10.1111/cup.14702\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>We recently read with great interest, the publication entitled “Granulomatous secondary syphilis: Another diagnostic pitfall for dermatopathologist” concerning a case of secondary syphilis with granulomatous inflammation on histopathology, which was immunohistochemically negative for <i>Treponema pallidum</i>.<span><sup>1</sup></span> Jin et al. underlined that granulomatous infiltration is uncommon in cases of secondary syphilis cutaneous lesions. In these cases, detecting the spirochetes may be difficult, as the number of microorganisms decreases in established, non-treated infections. Although the <i>T. pallidum</i> immunohistochemistry is highly sensitive and can detect even a small number of pathogens, the case described in the paper failed to stain. It was possible to establish the correct diagnosis by matching serological results.<span><sup>1</sup></span></p><p>Recently, a 48-year-old Caucasian woman visited our unit with a diffuse rash, which was present for 3 months without any other symptoms. The eruption consisted of widespread erythematous papules and nodules on the trunk and extremities without the involvement of the mucous membranes, palms, and soles (Figure 1A,B). She was referred to us by an external dermatologist with the suspected diagnosis of cutaneous lymphoma. The histopathological examination of a punch-biopsy specimen, a lesion on the left flank, revealed a granulomatous inflammatory infiltration in the dermis, with perivascular distribution (Figure 1C). At higher magnification, the epithelioid granulomas were surrounded by small lymphocytes and numerous plasma cells (Figure 1D). Immunohistochemistry for <i>T. pallidum</i> failed to reveal organisms. Despite the negativity of the stain, the histopathology was highly suspicious of secondary granulomatous syphilis; therefore, we suggested performing serological investigations to confirm the diagnosis of syphilis; both the Venereal Disease Research Laboratory and the <i>T. pallidum</i> hemagglutination assay (TPHA) were negative. The patient returned to us 3 weeks later due to the development of new lesions on the oral mucosa and a single lesion on the sole of the right foot. We decided to directly test for <i>T. pallidum</i> from an exudative lesion on the trunk using a real-time polymerase chain reaction (PCR) assay, which finally resulted in a positive detection. We repeated the serology in the Microbiology Laboratory of our Hospital on the same day of the cutaneous swab, and at this time, it resulted positive in syphilis, with a rapid plasma reagin (RPR) titer of 1:64 and a TPHA titer of 1:2560 and negative for HIV.</p><p>The patient received two intramuscular injections of 1 200 000 units of diaminocillin, preceded by 4 mg of betamethasone, resulting in complete remission of the disease.</p><p>Syphilis still represents a diagnostic pitfall for dermatologists and dermatopathologists, as it may manifest with a variety of clinical and histopathological features. From a clinical point-of-view, involvement of the palms and soles is typical of secondary syphilis. In cases of granulomatous syphilis, these sites are less commonly affected or may not be involved at all. Detecting the spirochetes using immunohistochemistry on the tissue samples may be challenging in these instances. The reason for this phenomenon is not clear, but it has been hypothesized that an impairment in the delayed-type hypersensitivity reaction, leading to chronic granulomatous inflammation, may be responsible.<span><sup>1</sup></span> In our case, the negativity for both treponemal and non-treponemal serological tests noticed the first time is explainable by the “hook effect” or “prozone phenomenon,” which is an immunological phenomenon whereby the immune complexes formation is impaired by the very high concentration of an antibody or an antigen, resulting in a false negative assay. This phenomenon has been reported in patients with HIV co-infection,<span><sup>2</sup></span> but it may occur also in patients with secondary syphilis characterized by a very high antibody titer.<span><sup>3</sup></span></p><p>Our case emphasizes the continued importance of conventional histology, based on hematoxylin–eosin in order to provide an accurate diagnosis. The presence of numerous plasma cells in the context of a granulomatous inflammation led us to be highly suspicious of secondary syphilis, even when both immunohistochemistry and serology were negative. In these cases, a PCR assay is helpful to confirm the diagnosis.<span><sup>4</sup></span> In fact, the negativity of the ancillary immunohistochemical techniques should not suggest the prompt exclusion of infectious diseases, especially in cases of granulomatous inflammation, when the microorganisms may be present in very small numbers. Moreover, serological tests may result in false negatives in some cases, therefore, RPR should be repeated with the diluted serum to reach a correct diagnosis and to avoid the “prozone phenomenon,” which contributes to misdiagnosis.</p>\",\"PeriodicalId\":15407,\"journal\":{\"name\":\"Journal of Cutaneous Pathology\",\"volume\":\"51 11\",\"pages\":\"866-867\"},\"PeriodicalIF\":1.6000,\"publicationDate\":\"2024-08-14\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1111/cup.14702\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Cutaneous Pathology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1111/cup.14702\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"DERMATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Cutaneous Pathology","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/cup.14702","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"DERMATOLOGY","Score":null,"Total":0}
Granulomatous secondary syphilis: When to maintain a high index of suspicion?
We recently read with great interest, the publication entitled “Granulomatous secondary syphilis: Another diagnostic pitfall for dermatopathologist” concerning a case of secondary syphilis with granulomatous inflammation on histopathology, which was immunohistochemically negative for Treponema pallidum.1 Jin et al. underlined that granulomatous infiltration is uncommon in cases of secondary syphilis cutaneous lesions. In these cases, detecting the spirochetes may be difficult, as the number of microorganisms decreases in established, non-treated infections. Although the T. pallidum immunohistochemistry is highly sensitive and can detect even a small number of pathogens, the case described in the paper failed to stain. It was possible to establish the correct diagnosis by matching serological results.1
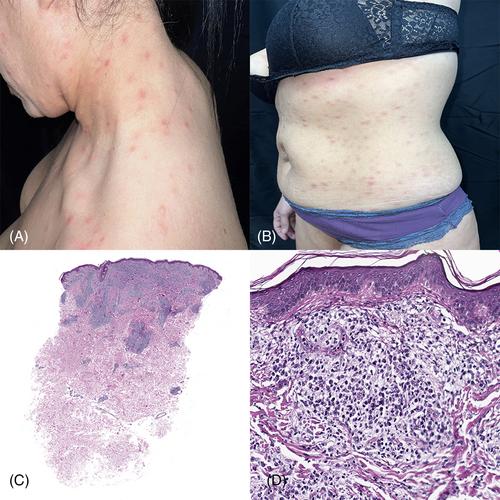
Recently, a 48-year-old Caucasian woman visited our unit with a diffuse rash, which was present for 3 months without any other symptoms. The eruption consisted of widespread erythematous papules and nodules on the trunk and extremities without the involvement of the mucous membranes, palms, and soles (Figure 1A,B). She was referred to us by an external dermatologist with the suspected diagnosis of cutaneous lymphoma. The histopathological examination of a punch-biopsy specimen, a lesion on the left flank, revealed a granulomatous inflammatory infiltration in the dermis, with perivascular distribution (Figure 1C). At higher magnification, the epithelioid granulomas were surrounded by small lymphocytes and numerous plasma cells (Figure 1D). Immunohistochemistry for T. pallidum failed to reveal organisms. Despite the negativity of the stain, the histopathology was highly suspicious of secondary granulomatous syphilis; therefore, we suggested performing serological investigations to confirm the diagnosis of syphilis; both the Venereal Disease Research Laboratory and the T. pallidum hemagglutination assay (TPHA) were negative. The patient returned to us 3 weeks later due to the development of new lesions on the oral mucosa and a single lesion on the sole of the right foot. We decided to directly test for T. pallidum from an exudative lesion on the trunk using a real-time polymerase chain reaction (PCR) assay, which finally resulted in a positive detection. We repeated the serology in the Microbiology Laboratory of our Hospital on the same day of the cutaneous swab, and at this time, it resulted positive in syphilis, with a rapid plasma reagin (RPR) titer of 1:64 and a TPHA titer of 1:2560 and negative for HIV.
The patient received two intramuscular injections of 1 200 000 units of diaminocillin, preceded by 4 mg of betamethasone, resulting in complete remission of the disease.
Syphilis still represents a diagnostic pitfall for dermatologists and dermatopathologists, as it may manifest with a variety of clinical and histopathological features. From a clinical point-of-view, involvement of the palms and soles is typical of secondary syphilis. In cases of granulomatous syphilis, these sites are less commonly affected or may not be involved at all. Detecting the spirochetes using immunohistochemistry on the tissue samples may be challenging in these instances. The reason for this phenomenon is not clear, but it has been hypothesized that an impairment in the delayed-type hypersensitivity reaction, leading to chronic granulomatous inflammation, may be responsible.1 In our case, the negativity for both treponemal and non-treponemal serological tests noticed the first time is explainable by the “hook effect” or “prozone phenomenon,” which is an immunological phenomenon whereby the immune complexes formation is impaired by the very high concentration of an antibody or an antigen, resulting in a false negative assay. This phenomenon has been reported in patients with HIV co-infection,2 but it may occur also in patients with secondary syphilis characterized by a very high antibody titer.3
Our case emphasizes the continued importance of conventional histology, based on hematoxylin–eosin in order to provide an accurate diagnosis. The presence of numerous plasma cells in the context of a granulomatous inflammation led us to be highly suspicious of secondary syphilis, even when both immunohistochemistry and serology were negative. In these cases, a PCR assay is helpful to confirm the diagnosis.4 In fact, the negativity of the ancillary immunohistochemical techniques should not suggest the prompt exclusion of infectious diseases, especially in cases of granulomatous inflammation, when the microorganisms may be present in very small numbers. Moreover, serological tests may result in false negatives in some cases, therefore, RPR should be repeated with the diluted serum to reach a correct diagnosis and to avoid the “prozone phenomenon,” which contributes to misdiagnosis.
期刊介绍:
Journal of Cutaneous Pathology publishes manuscripts broadly relevant to diseases of the skin and mucosae, with the aims of advancing scientific knowledge regarding dermatopathology and enhancing the communication between clinical practitioners and research scientists. Original scientific manuscripts on diagnostic and experimental cutaneous pathology are especially desirable. Timely, pertinent review articles also will be given high priority. Manuscripts based on light, fluorescence, and electron microscopy, histochemistry, immunology, molecular biology, and genetics, as well as allied sciences, are all welcome, provided their principal focus is on cutaneous pathology. Publication time will be kept as short as possible, ensuring that articles will be quickly available to all interested in this speciality.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


