{"title":"关于治疗转流性结肠炎和肠袋炎的最新综述,重点关注自体粪便微生物群移植的效用及其与肠道微生物群的关系。","authors":"Kentaro Tominaga, Yuichi Kojima, Yuzo Kawata, Kazuya Takahashi, Hiroki Sato, Atsunori Tsuchiya, Kenya Kamimura, Shuji Terai","doi":"10.12938/bmfh.2024-014","DOIUrl":null,"url":null,"abstract":"<p><p>Diversion colitis (DC) is characterized by mucosal inflammation in the defunctioned segment of the colon following a colostomy or ileostomy. The major causes of DC are an increase in the number of aerobic bacteria, a lack of short-chain fatty acids (SCFAs), and immune disorders in the diverted colon. However, its exact pathogenesis remains unknown. Various treatment strategies for DC have been explored, although none have been definitively established. Treatment approaches such as SCFAs, 5-aminosalicylic acid enemas, steroid enemas, and irrigation with fibers have been attempted, yielding various degrees of efficacies in mitigating mucosal inflammation. However, only individual case reports demonstrating the limited effect of the following therapies have been published: leukocytapheresis, dextrose (hypertonic glucose) spray, infliximab, an elemental diet, and coconut oil. The usefulness of probiotics for treating DC has recently been reported. Furthermore, fecal microbiota transplantation (FMT) has emerged as a promising treatment for DC. This review provides an update on the treatment strategies of DC, with a particular focus on FMT and its relationship with the intestinal microbiota. FMT may become the first choice of treatment for some patients in the future because of its low medical costs, ease of use, and minimal side effects. Furthermore, FMT can also be used for postoperative DC prophylaxis.</p>","PeriodicalId":93908,"journal":{"name":"Bioscience of microbiota, food and health","volume":"43 3","pages":"162-169"},"PeriodicalIF":2.9000,"publicationDate":"2024-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11220330/pdf/","citationCount":"0","resultStr":"{\"title\":\"An updated review on the treatment for diversion colitis and pouchitis, with a focus on the utility of autologous fecal microbiota transplantation and its relationship with the intestinal microbiota.\",\"authors\":\"Kentaro Tominaga, Yuichi Kojima, Yuzo Kawata, Kazuya Takahashi, Hiroki Sato, Atsunori Tsuchiya, Kenya Kamimura, Shuji Terai\",\"doi\":\"10.12938/bmfh.2024-014\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Diversion colitis (DC) is characterized by mucosal inflammation in the defunctioned segment of the colon following a colostomy or ileostomy. The major causes of DC are an increase in the number of aerobic bacteria, a lack of short-chain fatty acids (SCFAs), and immune disorders in the diverted colon. However, its exact pathogenesis remains unknown. Various treatment strategies for DC have been explored, although none have been definitively established. Treatment approaches such as SCFAs, 5-aminosalicylic acid enemas, steroid enemas, and irrigation with fibers have been attempted, yielding various degrees of efficacies in mitigating mucosal inflammation. However, only individual case reports demonstrating the limited effect of the following therapies have been published: leukocytapheresis, dextrose (hypertonic glucose) spray, infliximab, an elemental diet, and coconut oil. The usefulness of probiotics for treating DC has recently been reported. Furthermore, fecal microbiota transplantation (FMT) has emerged as a promising treatment for DC. This review provides an update on the treatment strategies of DC, with a particular focus on FMT and its relationship with the intestinal microbiota. FMT may become the first choice of treatment for some patients in the future because of its low medical costs, ease of use, and minimal side effects. Furthermore, FMT can also be used for postoperative DC prophylaxis.</p>\",\"PeriodicalId\":93908,\"journal\":{\"name\":\"Bioscience of microbiota, food and health\",\"volume\":\"43 3\",\"pages\":\"162-169\"},\"PeriodicalIF\":2.9000,\"publicationDate\":\"2024-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11220330/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Bioscience of microbiota, food and health\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.12938/bmfh.2024-014\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/4/23 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"MICROBIOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Bioscience of microbiota, food and health","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.12938/bmfh.2024-014","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/4/23 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"MICROBIOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
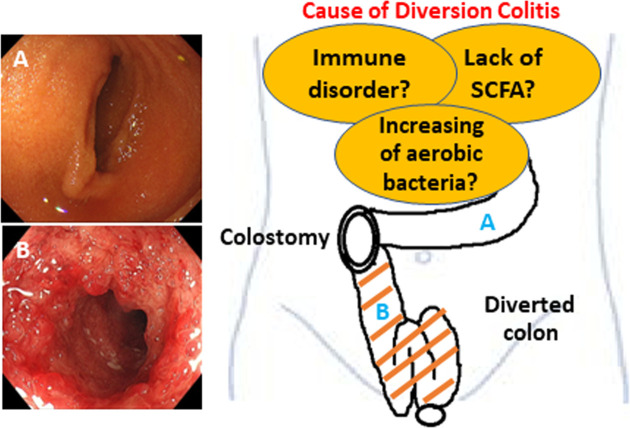
转流性结肠炎(DC)的特征是结肠造口术或回肠造口术后失去功能的结肠段出现粘膜炎症。引起转流性结肠炎的主要原因是需氧细菌数量增加、短链脂肪酸(SCFA)缺乏以及转流结肠的免疫紊乱。然而,其确切的发病机制仍不清楚。人们探索了各种治疗 DC 的策略,但都没有得到明确证实。已尝试过的治疗方法包括 SCFAs、5-氨基水杨酸灌肠、类固醇灌肠和纤维灌肠,在减轻粘膜炎症方面取得了不同程度的疗效。然而,只有个别病例报告显示以下疗法的效果有限:白细胞清除术、葡萄糖(高渗葡萄糖)喷雾剂、英夫利昔单抗、元素饮食和椰子油。最近有报道称益生菌可用于治疗 DC。此外,粪便微生物群移植(FMT)已成为一种很有前景的 DC 治疗方法。本综述介绍了 DC 治疗策略的最新进展,尤其侧重于 FMT 及其与肠道微生物群的关系。由于 FMT 医疗费用低廉、易于使用且副作用极小,未来可能会成为一些患者的首选治疗方法。此外,FMT 还可用于 DC 术后预防。
An updated review on the treatment for diversion colitis and pouchitis, with a focus on the utility of autologous fecal microbiota transplantation and its relationship with the intestinal microbiota.
Diversion colitis (DC) is characterized by mucosal inflammation in the defunctioned segment of the colon following a colostomy or ileostomy. The major causes of DC are an increase in the number of aerobic bacteria, a lack of short-chain fatty acids (SCFAs), and immune disorders in the diverted colon. However, its exact pathogenesis remains unknown. Various treatment strategies for DC have been explored, although none have been definitively established. Treatment approaches such as SCFAs, 5-aminosalicylic acid enemas, steroid enemas, and irrigation with fibers have been attempted, yielding various degrees of efficacies in mitigating mucosal inflammation. However, only individual case reports demonstrating the limited effect of the following therapies have been published: leukocytapheresis, dextrose (hypertonic glucose) spray, infliximab, an elemental diet, and coconut oil. The usefulness of probiotics for treating DC has recently been reported. Furthermore, fecal microbiota transplantation (FMT) has emerged as a promising treatment for DC. This review provides an update on the treatment strategies of DC, with a particular focus on FMT and its relationship with the intestinal microbiota. FMT may become the first choice of treatment for some patients in the future because of its low medical costs, ease of use, and minimal side effects. Furthermore, FMT can also be used for postoperative DC prophylaxis.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


