Alasdair G Rooney, William Hewins, Amie Walker, Mairi Mackinnon, Lisa Withington, Sara Robson, Claire Torrens, Lisa E M Hopcroft, Antony Clark, Garry Anderson, Helen Bulbeck, Joanna Dunlop, Michelle Welsh, Aimee Dyson, Julie Emerson, Carol Cochrane, Robert Hill, Jade Carruthers, Julia Day, David Gillespie, Christopher Hewitt, Emanuela Molinari, Mary Wells, Catherine McBain, Anthony J Chalmers, Robin Grant
{"title":"Lifestyle coaching is feasible in fatigued brain tumor patients: A phase I/feasibility, multi-center, mixed-methods randomized controlled trial.","authors":"Alasdair G Rooney, William Hewins, Amie Walker, Mairi Mackinnon, Lisa Withington, Sara Robson, Claire Torrens, Lisa E M Hopcroft, Antony Clark, Garry Anderson, Helen Bulbeck, Joanna Dunlop, Michelle Welsh, Aimee Dyson, Julie Emerson, Carol Cochrane, Robert Hill, Jade Carruthers, Julia Day, David Gillespie, Christopher Hewitt, Emanuela Molinari, Mary Wells, Catherine McBain, Anthony J Chalmers, Robin Grant","doi":"10.1093/nop/npac086","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>There are no effective treatments for brain tumor-related fatigue. We studied the feasibility of two novel lifestyle coaching interventions in fatigued brain tumor patients.</p><p><strong>Methods: </strong>This phase I/feasibility multi-center RCT recruited patients with a clinically stable primary brain tumor and significant fatigue (mean Brief Fatigue Inventory [BFI] score ≥ 4/10). Participants were randomized in a 1-1-1 allocation ratio to: Control (usual care); Health Coaching (\"HC\", an eight-week program targeting lifestyle behaviors); or HC plus Activation Coaching (\"HC + AC\", further targeting self-efficacy). The primary outcome was feasibility of recruitment and retention. Secondary outcomes were intervention acceptability, which was evaluated via qualitative interview, and safety. Exploratory quantitative outcomes were measured at baseline (T0), post-interventions (T1, 10 weeks), and endpoint (T2, 16 weeks).</p><p><strong>Results: </strong><i>n</i> = 46 fatigued brain tumor patients (T0 BFI mean = 6.8/10) were recruited and 34 were retained to endpoint, establishing feasibility. Engagement with interventions was sustained over time. Qualitative interviews (<i>n</i> = 21) suggested that coaching interventions were broadly acceptable, although mediated by participant outlook and prior lifestyle. Coaching led to significant improvements in fatigue (improvement in BFI versus control at T1: HC=2.2 points [95% CI 0.6, 3.8], HC + AC = 1.8 [0.1, 3.4], Cohen's <i>d</i> [HC] = 1.9; improvement in FACIT-Fatigue: HC = 4.8 points [-3.7, 13.3]; HC + AC = 12 [3.5, 20.5], <i>d</i> [HC and AC] = 0.9). Coaching also improved depressive and mental health outcomes. Modeling suggested a potential limiting effect of higher baseline depressive symptoms.</p><p><strong>Conclusions: </strong>Lifestyle coaching interventions are feasible to deliver to fatigued brain tumor patients. They were manageable, acceptable, and safe, with preliminary evidence of benefit on fatigue and mental health outcomes. Larger trials of efficacy are justified.</p>","PeriodicalId":19234,"journal":{"name":"Neuro-oncology practice","volume":"10 3","pages":"249-260"},"PeriodicalIF":2.4000,"publicationDate":"2022-10-14","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10180387/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Neuro-oncology practice","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/nop/npac086","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/6/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: There are no effective treatments for brain tumor-related fatigue. We studied the feasibility of two novel lifestyle coaching interventions in fatigued brain tumor patients.
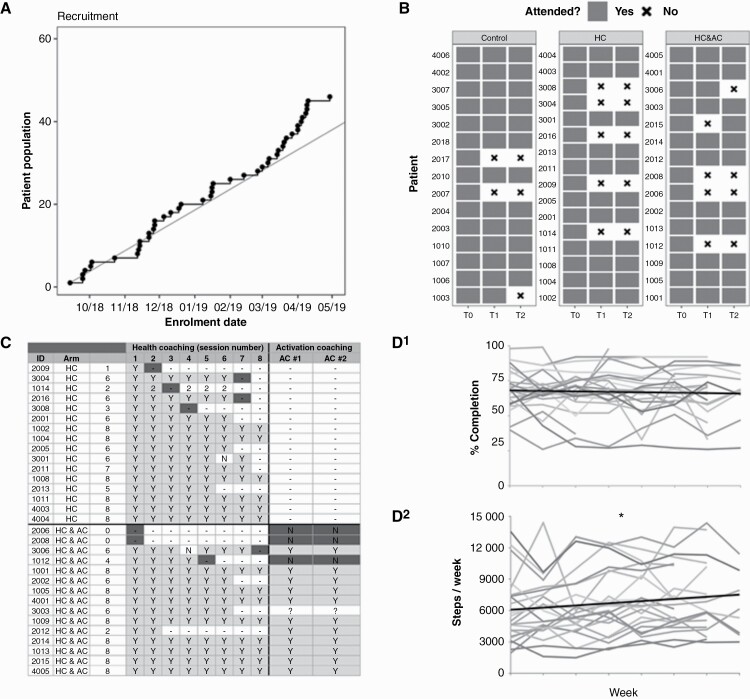
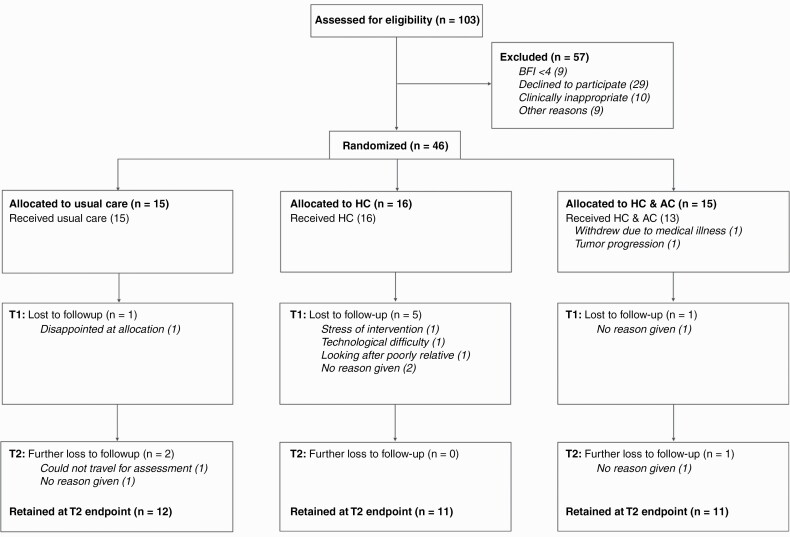
Methods: This phase I/feasibility multi-center RCT recruited patients with a clinically stable primary brain tumor and significant fatigue (mean Brief Fatigue Inventory [BFI] score ≥ 4/10). Participants were randomized in a 1-1-1 allocation ratio to: Control (usual care); Health Coaching ("HC", an eight-week program targeting lifestyle behaviors); or HC plus Activation Coaching ("HC + AC", further targeting self-efficacy). The primary outcome was feasibility of recruitment and retention. Secondary outcomes were intervention acceptability, which was evaluated via qualitative interview, and safety. Exploratory quantitative outcomes were measured at baseline (T0), post-interventions (T1, 10 weeks), and endpoint (T2, 16 weeks).
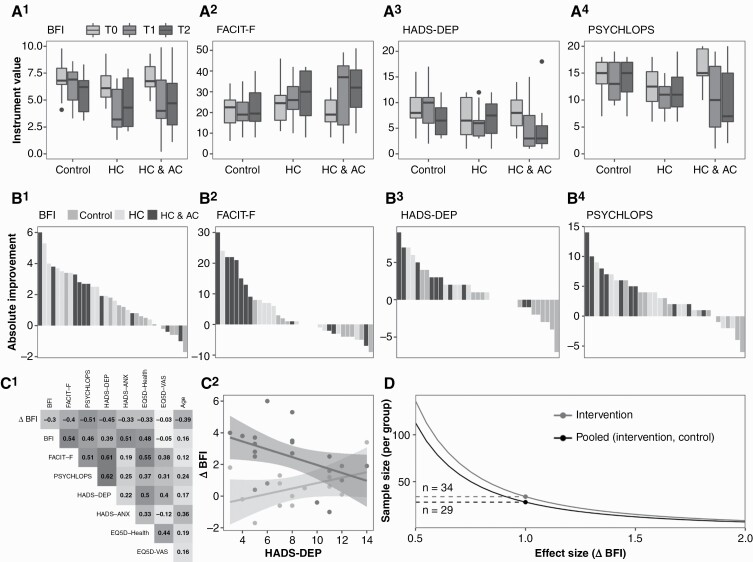
Results: n = 46 fatigued brain tumor patients (T0 BFI mean = 6.8/10) were recruited and 34 were retained to endpoint, establishing feasibility. Engagement with interventions was sustained over time. Qualitative interviews (n = 21) suggested that coaching interventions were broadly acceptable, although mediated by participant outlook and prior lifestyle. Coaching led to significant improvements in fatigue (improvement in BFI versus control at T1: HC=2.2 points [95% CI 0.6, 3.8], HC + AC = 1.8 [0.1, 3.4], Cohen's d [HC] = 1.9; improvement in FACIT-Fatigue: HC = 4.8 points [-3.7, 13.3]; HC + AC = 12 [3.5, 20.5], d [HC and AC] = 0.9). Coaching also improved depressive and mental health outcomes. Modeling suggested a potential limiting effect of higher baseline depressive symptoms.
Conclusions: Lifestyle coaching interventions are feasible to deliver to fatigued brain tumor patients. They were manageable, acceptable, and safe, with preliminary evidence of benefit on fatigue and mental health outcomes. Larger trials of efficacy are justified.
期刊介绍:
Neuro-Oncology Practice focuses on the clinical aspects of the subspecialty for practicing clinicians and healthcare specialists from a variety of disciplines including physicians, nurses, physical/occupational therapists, neuropsychologists, and palliative care specialists, who have focused their careers on clinical patient care and who want to apply the latest treatment advances to their practice. These include: Applying new trial results to improve standards of patient care Translating scientific advances such as tumor molecular profiling and advanced imaging into clinical treatment decision making and personalized brain tumor therapies Raising awareness of basic, translational and clinical research in areas of symptom management, survivorship, neurocognitive function, end of life issues and caregiving

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


