Sina Burth, Jan Meis, Dorothea Kronsteiner, Helena Heckhausen, Klaus Zweckberger, Meinhard Kieser, Wolfgang Wick, Christian Ulfert, Markus Möhlenbruch, Peter Ringleb, Silvia Schönenberger
{"title":"Outcome analysis for patients with subarachnoid hemorrhage and vasospasm including endovascular treatment.","authors":"Sina Burth, Jan Meis, Dorothea Kronsteiner, Helena Heckhausen, Klaus Zweckberger, Meinhard Kieser, Wolfgang Wick, Christian Ulfert, Markus Möhlenbruch, Peter Ringleb, Silvia Schönenberger","doi":"10.1186/s42466-023-00283-3","DOIUrl":null,"url":null,"abstract":"<p><p>As a complication of subarachnoid hemorrhage (SAH), vasospasm substantially contributes to its morbidity and mortality. We aimed at analyzing predictors of outcome for these patients including the role of endovascular treatment (ET). Our database was screened for patients with SAH treated in our Neuro-ICU from 2009 to 2019. Clinical parameters including functional outcome (modified Rankin Scale, mRS of 0-2 or 3-6 at discharge and after a median follow-up of 18 months) and details about ET were gathered on 465 patients, 241 (52%) of whom experienced vasospasm. Descriptive analyses were performed to identify explanatory variables for the dichotomized mRS score. A logistic regression model was fitted on 241 patients with vasospasm including age, Hunt and Hess Score, extraventricular drainage (EVD), forced hypertension, ET and delayed cerebral ischemia (DCI). The model found a Hunt and Hess Score of 5 (OR = 0.043, p = 0.008), requirement of EVD (OR = 0.161, p < 0.001), forced hypertension (OR = 0.242, p = 0.001), ET (OR = 0.431, p = 0.043) and DCI (OR = 0.229, p < 0.001) to be negative predictors of outcome while age was not. Use of intraarterial nimodipine alone (OR = 0.778, p = 0.705) or including balloon angioplasty (OR = 0.894, p = 0.902) and number of ETs per patient (OR = 0.757, p = 0.416) were not significant in a separate model with otherwise identical variables. While DCI is clearly associated with poor outcome, the influence of ET on outcome remains inconclusive. Limited by their retrospective nature and an indication bias, these data encourage a randomized assessment of ET.</p>","PeriodicalId":94156,"journal":{"name":"Neurological research and practice","volume":"5 1","pages":"57"},"PeriodicalIF":0.0000,"publicationDate":"2023-11-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10621117/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Neurological research and practice","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s42466-023-00283-3","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
Abstract
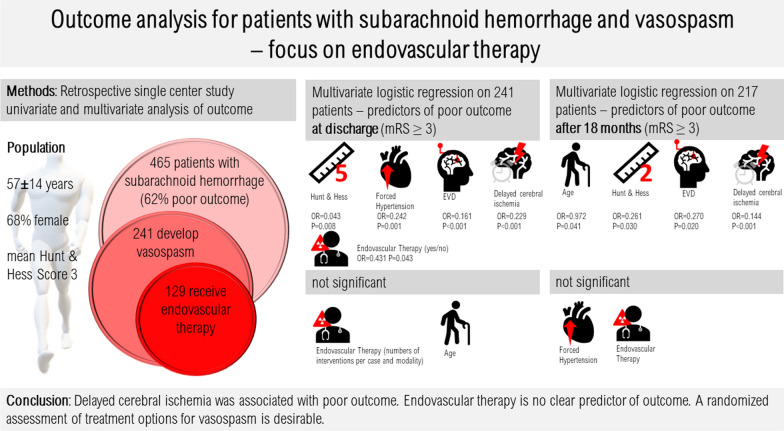
As a complication of subarachnoid hemorrhage (SAH), vasospasm substantially contributes to its morbidity and mortality. We aimed at analyzing predictors of outcome for these patients including the role of endovascular treatment (ET). Our database was screened for patients with SAH treated in our Neuro-ICU from 2009 to 2019. Clinical parameters including functional outcome (modified Rankin Scale, mRS of 0-2 or 3-6 at discharge and after a median follow-up of 18 months) and details about ET were gathered on 465 patients, 241 (52%) of whom experienced vasospasm. Descriptive analyses were performed to identify explanatory variables for the dichotomized mRS score. A logistic regression model was fitted on 241 patients with vasospasm including age, Hunt and Hess Score, extraventricular drainage (EVD), forced hypertension, ET and delayed cerebral ischemia (DCI). The model found a Hunt and Hess Score of 5 (OR = 0.043, p = 0.008), requirement of EVD (OR = 0.161, p < 0.001), forced hypertension (OR = 0.242, p = 0.001), ET (OR = 0.431, p = 0.043) and DCI (OR = 0.229, p < 0.001) to be negative predictors of outcome while age was not. Use of intraarterial nimodipine alone (OR = 0.778, p = 0.705) or including balloon angioplasty (OR = 0.894, p = 0.902) and number of ETs per patient (OR = 0.757, p = 0.416) were not significant in a separate model with otherwise identical variables. While DCI is clearly associated with poor outcome, the influence of ET on outcome remains inconclusive. Limited by their retrospective nature and an indication bias, these data encourage a randomized assessment of ET.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


