Enrico Cocchi, Silvia Bloise, Aurora Lorefice, Sara Zannoni, Benedetta Pellegrini, Francesco Saverio Morlupo, Beatrice Scarpellini, Melodie Olivia Loredana Rosa Aricò, Francesco Accomando, Gina Ancora, Gianluca Vergine, Enrico Valletta, Marcello Stella, Federico Marchetti
{"title":"Multicentre study on nirsevimab: Bayesian analysis reveals persisting risk for preterm infants.","authors":"Enrico Cocchi, Silvia Bloise, Aurora Lorefice, Sara Zannoni, Benedetta Pellegrini, Francesco Saverio Morlupo, Beatrice Scarpellini, Melodie Olivia Loredana Rosa Aricò, Francesco Accomando, Gina Ancora, Gianluca Vergine, Enrico Valletta, Marcello Stella, Federico Marchetti","doi":"10.1136/bmjpo-2025-003665","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>To evaluate whether the timing and effectiveness of nirsevimab prophylaxis vary by gestational age.</p><p><strong>Design: </strong>Retrospective cohort study conducted during two identical epidemic seasons: 2023-2024 (before nirsevimab introduction) and 2024-2025 (after nirsevimab introduction).</p><p><strong>Setting: </strong>Multicentre study involving five hospitals in Italy.</p><p><strong>Patients: </strong>All infants under 1 year of age hospitalised for acute lower respiratory tract infection across two consecutive respiratory syncytial virus (RSV) seasons. We compared the number of RSV-positive hospitalisations (283 cases) and, among those admissions, clinical severity between the pre-nirsevimab and post-nirsevimab seasons, given live birth denominators at participating hospitals were stable. RSV-negative hospitalisations (79 cases) were analysed in parallel as a sensitivity analysis.</p><p><strong>Intervention: </strong>The study compared hospitalised infants eligible for RSV immunoprophylaxis during the 2024-2025 season who received nirsevimab, with those from the 2023-2024 season who did not receive nirsevimab (or received palivizumab, if indicated).</p><p><strong>Main outcome measures: </strong>The primary outcome was the count of RSV-associated hospitalisation, with nirsevimab prophylaxis as the primary exposure, considering live birth denominators at participating hospitals were stable. Particular attention was given to whether gestational age modified the effectiveness of the prophylaxis. Secondary outcomes included measures of disease severity (eg, high-flow nasal cannula use, neonatal intensive care unit admission), adjusted for the effect of gestational age and other relevant covariates. Bayesian hierarchical regression models were used, with sensitivity analyses performed both in negative cases and using frequentist bootstrapped hierarchical models.</p><p><strong>Results: </strong>Median gestational age at birth was 39.7 (38.7-40.7) weeks in the no-prophylaxis group versus 37.3 (35.3-39.0) weeks in the nirsevimab group. Despite prophylaxis, lower gestational age was associated with an increased risk of hospitalisation (Bayesian posterior probability, 98.68%; maximum a posteriori HR 0.63; 95% highest density interval: 0.41-0.95). No RSV hospitalisations occurred between 40 and 90 days post-prophylaxis, suggesting a window of maximal effectiveness. Nirsevimab significantly reduced RSV-related hospitalisations and the need for non-invasive respiratory support.</p><p><strong>Conclusions: </strong>Nirsevimab prophylaxis was associated with reduced hospitalisation and severity. However, protection waned in preterm infants, highlighting the need to investigate modified dosing strategies for this high-risk population.</p>","PeriodicalId":9069,"journal":{"name":"BMJ Paediatrics Open","volume":"9 1","pages":""},"PeriodicalIF":2.3000,"publicationDate":"2025-10-14","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12519650/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMJ Paediatrics Open","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1136/bmjpo-2025-003665","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"PEDIATRICS","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: To evaluate whether the timing and effectiveness of nirsevimab prophylaxis vary by gestational age.
Design: Retrospective cohort study conducted during two identical epidemic seasons: 2023-2024 (before nirsevimab introduction) and 2024-2025 (after nirsevimab introduction).
Setting: Multicentre study involving five hospitals in Italy.
Patients: All infants under 1 year of age hospitalised for acute lower respiratory tract infection across two consecutive respiratory syncytial virus (RSV) seasons. We compared the number of RSV-positive hospitalisations (283 cases) and, among those admissions, clinical severity between the pre-nirsevimab and post-nirsevimab seasons, given live birth denominators at participating hospitals were stable. RSV-negative hospitalisations (79 cases) were analysed in parallel as a sensitivity analysis.
Intervention: The study compared hospitalised infants eligible for RSV immunoprophylaxis during the 2024-2025 season who received nirsevimab, with those from the 2023-2024 season who did not receive nirsevimab (or received palivizumab, if indicated).
Main outcome measures: The primary outcome was the count of RSV-associated hospitalisation, with nirsevimab prophylaxis as the primary exposure, considering live birth denominators at participating hospitals were stable. Particular attention was given to whether gestational age modified the effectiveness of the prophylaxis. Secondary outcomes included measures of disease severity (eg, high-flow nasal cannula use, neonatal intensive care unit admission), adjusted for the effect of gestational age and other relevant covariates. Bayesian hierarchical regression models were used, with sensitivity analyses performed both in negative cases and using frequentist bootstrapped hierarchical models.
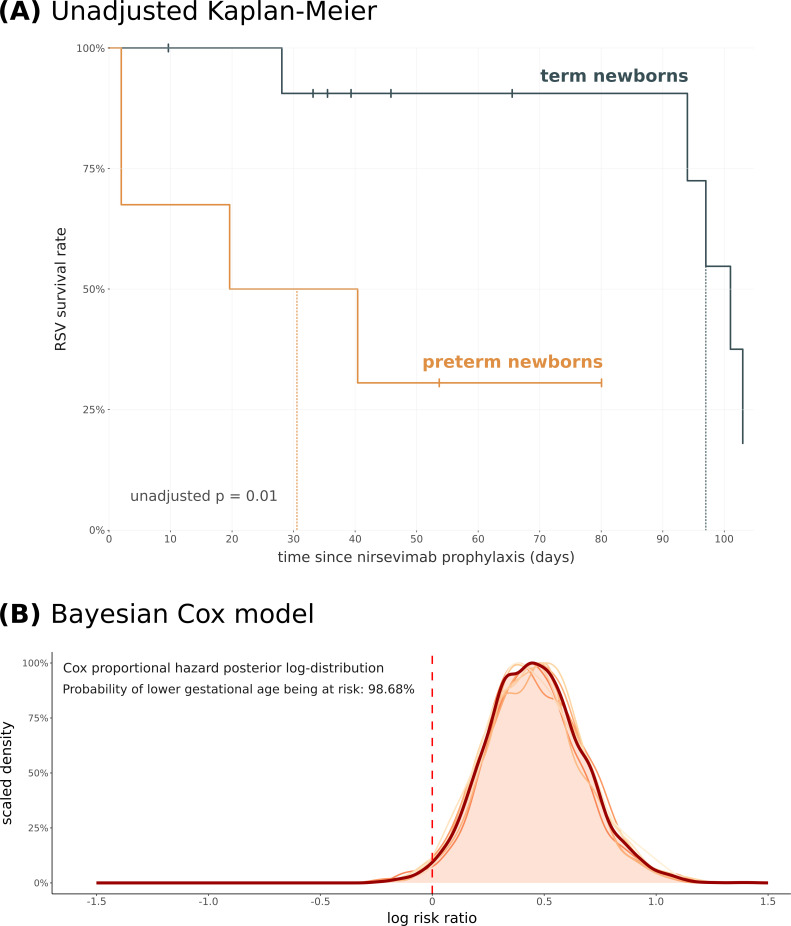
Results: Median gestational age at birth was 39.7 (38.7-40.7) weeks in the no-prophylaxis group versus 37.3 (35.3-39.0) weeks in the nirsevimab group. Despite prophylaxis, lower gestational age was associated with an increased risk of hospitalisation (Bayesian posterior probability, 98.68%; maximum a posteriori HR 0.63; 95% highest density interval: 0.41-0.95). No RSV hospitalisations occurred between 40 and 90 days post-prophylaxis, suggesting a window of maximal effectiveness. Nirsevimab significantly reduced RSV-related hospitalisations and the need for non-invasive respiratory support.
Conclusions: Nirsevimab prophylaxis was associated with reduced hospitalisation and severity. However, protection waned in preterm infants, highlighting the need to investigate modified dosing strategies for this high-risk population.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


