Shin-Jae Kim, Pratyush Shahi, Sang-Ho Lee, Junseok Bae
{"title":"Long-term Outcomes of Multilevel Anterior Cervical Osteotomy and Posterior Instrumentation for OPLL-Induced Myelopathy With Cervical Kyphosis.","authors":"Shin-Jae Kim, Pratyush Shahi, Sang-Ho Lee, Junseok Bae","doi":"10.14245/ns.2550256.128","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>To analyze long-term clinical and radiological outcomes after multilevel anterior osteotomy with posterior instrumentation in patients with ossification of posterior longitudinal ligament (OPLL)-induced myelopathy and cervical kyphosis.</p><p><strong>Methods: </strong>Patients who underwent multilevel anterior osteotomy with posterior instrumentation for OPLL-induced myelopathy and cervical kyphosis and had a minimum of 5-year follow-up were included. Clinical outcomes (Japanese Orthopaedic Association score system for cervical myelopathy [C-JOA], 12-item Short Form health survey [SF-12], Neck Disability Index [NDI]) and radiological parameters (C2-7 lordosis, center of gravity of the head [CGH]-C7 sagittal vertical axis [SVA], T1 slope) were analyzed at the preoperative, immediate postoperative, and latest follow-up timepoints.</p><p><strong>Results: </strong>Twenty-eight patients were included. The average follow-up period was 66.4 months. All clinical outcome parameters showed significant improvement. C-JOA, SF-12, and NDI showed significant improvement at latest follow-up (p<0.001). C2-7 lordosis increased significantly immediately postoperatively (-6.0°±10.4°) compared to preoperatively (+9.2°±9.6°), and was largely maintained at latest follow-up (-5.7°±9.4°). T1 slope significantly increased between the immediate postoperative timepoint (21.9°±7.7°) and latest follow-up (24.2°±9.5°) (p=0.046). CGH-C7 SVA significantly increased between the immediate postoperative timepoint (22.7±14.8 mm) and latest follow-up (32.2±22.6 mm) (p=0.046).</p><p><strong>Conclusion: </strong>Multilevel anterior osteotomy with posterior instrumentation is a safe and effective surgical option for OPLL-induced myelopathy with kyphotic cervical alignment. Future studies are required to investigate the forward tilting of cervical spine over time after surgery.</p>","PeriodicalId":19269,"journal":{"name":"Neurospine","volume":"22 3","pages":"623-630"},"PeriodicalIF":3.6000,"publicationDate":"2025-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12518910/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Neurospine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.14245/ns.2550256.128","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/9/30 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: To analyze long-term clinical and radiological outcomes after multilevel anterior osteotomy with posterior instrumentation in patients with ossification of posterior longitudinal ligament (OPLL)-induced myelopathy and cervical kyphosis.
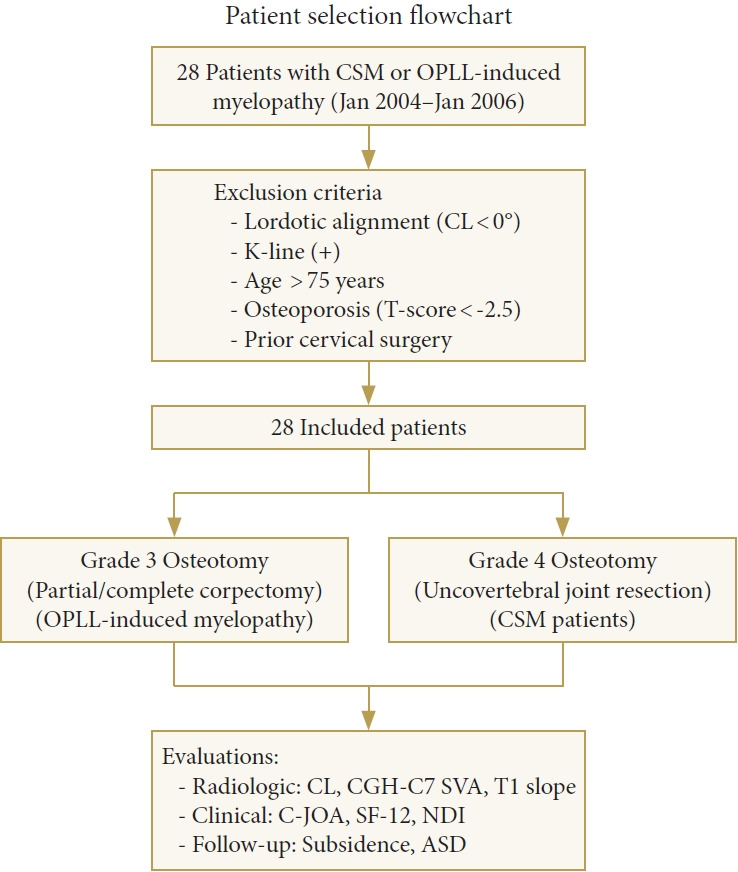
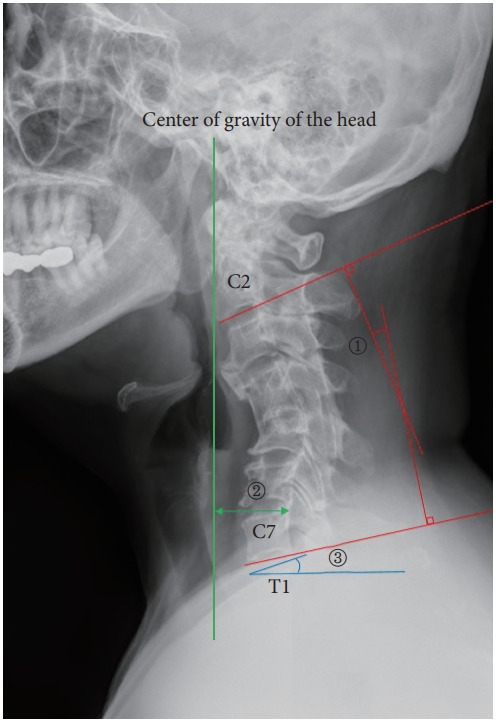
Methods: Patients who underwent multilevel anterior osteotomy with posterior instrumentation for OPLL-induced myelopathy and cervical kyphosis and had a minimum of 5-year follow-up were included. Clinical outcomes (Japanese Orthopaedic Association score system for cervical myelopathy [C-JOA], 12-item Short Form health survey [SF-12], Neck Disability Index [NDI]) and radiological parameters (C2-7 lordosis, center of gravity of the head [CGH]-C7 sagittal vertical axis [SVA], T1 slope) were analyzed at the preoperative, immediate postoperative, and latest follow-up timepoints.
Results: Twenty-eight patients were included. The average follow-up period was 66.4 months. All clinical outcome parameters showed significant improvement. C-JOA, SF-12, and NDI showed significant improvement at latest follow-up (p<0.001). C2-7 lordosis increased significantly immediately postoperatively (-6.0°±10.4°) compared to preoperatively (+9.2°±9.6°), and was largely maintained at latest follow-up (-5.7°±9.4°). T1 slope significantly increased between the immediate postoperative timepoint (21.9°±7.7°) and latest follow-up (24.2°±9.5°) (p=0.046). CGH-C7 SVA significantly increased between the immediate postoperative timepoint (22.7±14.8 mm) and latest follow-up (32.2±22.6 mm) (p=0.046).
Conclusion: Multilevel anterior osteotomy with posterior instrumentation is a safe and effective surgical option for OPLL-induced myelopathy with kyphotic cervical alignment. Future studies are required to investigate the forward tilting of cervical spine over time after surgery.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


