Hangeul Park, Woojin Kim, Jungbo Sim, Ho Sung Myeong, Young Doo Choi, Gilho Kwak, Bo Eun Kim, Jeongeum Park, Sung-Min Kim, Keewon Kim, Hee-Pyoung Park, Jun-Hoe Kim, Chang-Hyun Lee, Chun Kee Chung, Chi Heon Kim
{"title":"The Role of D-Wave Monitoring in Motor-Evoked Potential Loss During Intramedullary Spinal Cord Tumors Resection.","authors":"Hangeul Park, Woojin Kim, Jungbo Sim, Ho Sung Myeong, Young Doo Choi, Gilho Kwak, Bo Eun Kim, Jeongeum Park, Sung-Min Kim, Keewon Kim, Hee-Pyoung Park, Jun-Hoe Kim, Chang-Hyun Lee, Chun Kee Chung, Chi Heon Kim","doi":"10.14245/ns.2550594.297","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>Motor-evoked potential (MEP) loss during intramedullary (IM) spinal cord tumor surgery impairs the ability to monitor further neural injury. Direct wave (D-wave) monitoring may allow continued assessment of corticospinal tract integrity after MEP loss. This study evaluates the role of D-wave-guided surgery in preserving function and enabling safe resection after MEP loss.</p><p><strong>Methods: </strong>A retrospective study was conducted in adult patients with ependymoma (EPN), cavernous angioma (CA) or subependymoma who experienced MEP loss during IM tumor resection between January 2012 and May 2025. Patients who underwent continued resection under D-wave guidance after MEP loss were compared with those who did not.</p><p><strong>Results: </strong>Among 37 eligible patients, 9 underwent D-wave-guided surgery and 28 did not. Functional improvement at the last follow-up was more frequent in the D-wave-guided surgery group (66.7% vs. 17.9%, p=0.011). This trend remained significant in EPN patients (74.4% vs. 9.1%, p=0.003), but not in CA patients. Immediate postoperative motor grade ≤3 was more common in the D-wave-guided surgery group (66.7% vs. 39.3%), although this difference was not statistically significant (p=0.251). By last follow-up, the proportions of patients self-ambulatory without external aids (88.9% vs. 89.3%, p=1.000) were similar between groups. Extent of resection, complications, and recurrence rates showed no significant differences.</p><p><strong>Conclusion: </strong>D-wave-guided surgery may enable safe continuation of tumor resection after MEP loss without increasing morbidity. It offers a viable intraoperative strategy to preserve long-term motor function by extending monitoring beyond MEP limitations.</p>","PeriodicalId":19269,"journal":{"name":"Neurospine","volume":"22 3","pages":"650-662"},"PeriodicalIF":3.6000,"publicationDate":"2025-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12518915/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Neurospine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.14245/ns.2550594.297","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/9/30 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: Motor-evoked potential (MEP) loss during intramedullary (IM) spinal cord tumor surgery impairs the ability to monitor further neural injury. Direct wave (D-wave) monitoring may allow continued assessment of corticospinal tract integrity after MEP loss. This study evaluates the role of D-wave-guided surgery in preserving function and enabling safe resection after MEP loss.
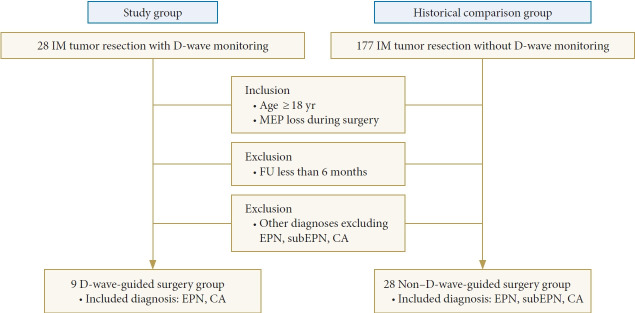
Methods: A retrospective study was conducted in adult patients with ependymoma (EPN), cavernous angioma (CA) or subependymoma who experienced MEP loss during IM tumor resection between January 2012 and May 2025. Patients who underwent continued resection under D-wave guidance after MEP loss were compared with those who did not.
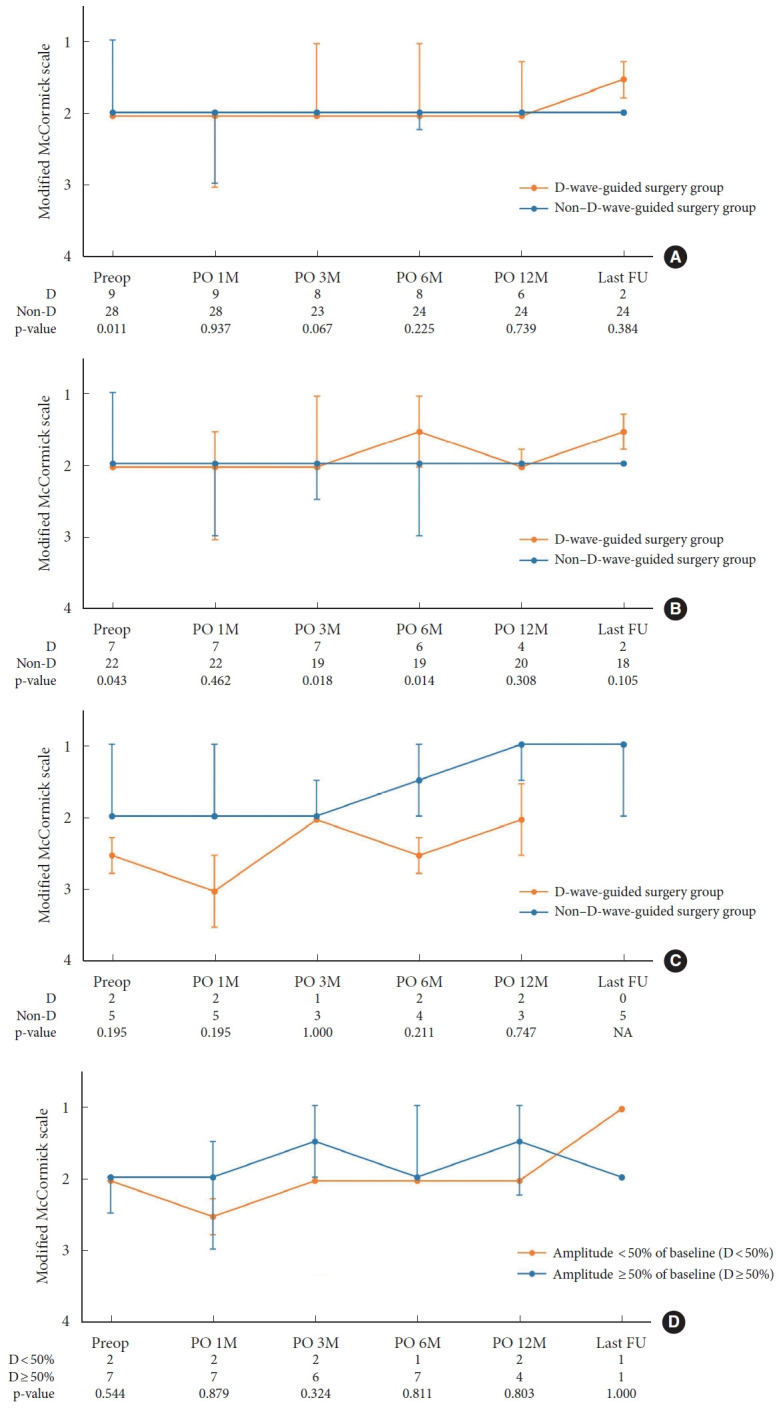
Results: Among 37 eligible patients, 9 underwent D-wave-guided surgery and 28 did not. Functional improvement at the last follow-up was more frequent in the D-wave-guided surgery group (66.7% vs. 17.9%, p=0.011). This trend remained significant in EPN patients (74.4% vs. 9.1%, p=0.003), but not in CA patients. Immediate postoperative motor grade ≤3 was more common in the D-wave-guided surgery group (66.7% vs. 39.3%), although this difference was not statistically significant (p=0.251). By last follow-up, the proportions of patients self-ambulatory without external aids (88.9% vs. 89.3%, p=1.000) were similar between groups. Extent of resection, complications, and recurrence rates showed no significant differences.
Conclusion: D-wave-guided surgery may enable safe continuation of tumor resection after MEP loss without increasing morbidity. It offers a viable intraoperative strategy to preserve long-term motor function by extending monitoring beyond MEP limitations.
目的:髓内(IM)脊髓肿瘤手术中运动诱发电位(MEP)的丢失损害了进一步神经损伤的监测能力。直接波(d波)监测可以在MEP丧失后继续评估皮质脊髓束完整性。本研究评估了d波引导手术在MEP丢失后保留功能和实现安全切除中的作用。方法:回顾性研究了2012年1月至2025年5月期间在IM肿瘤切除术中发生MEP丢失的成年室管膜瘤(EPN)、海绵状血管瘤(CA)或室管膜下瘤患者。对MEP丢失后在d波引导下继续切除的患者进行比较。结果:在37例符合条件的患者中,9例接受了d波引导手术,28例未接受手术。最后一次随访时,d波引导手术组功能改善更频繁(66.7% vs. 17.9%, p=0.011)。这一趋势在EPN患者中仍然显著(74.4% vs. 9.1%, p=0.003),但在CA患者中不明显。d波引导手术组术后立即运动等级≤3级更常见(66.7%比39.3%),但差异无统计学意义(p=0.251)。末次随访时,两组患者无辅助设备自行走动的比例(88.9% vs 89.3%, p=1.000)相似。手术切除程度、并发症及复发率无明显差异。结论:d波引导手术可以使MEP丢失后的肿瘤安全继续切除,而不会增加发病率。它提供了一种可行的术中策略,通过延长MEP限制的监测来保持长期的运动功能。

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


