Sang Hoon Hwang, Seung Jun Ryu, Min Han Kim, Jong Koo Lee, Sun Woo Jang, Danbi Park, Chong Man Kim, Jin Hoon Park
{"title":"Atlantoaxial Reconstruction: The Artful Evolution of Craniovertebral Junctional Spine Surgery.","authors":"Sang Hoon Hwang, Seung Jun Ryu, Min Han Kim, Jong Koo Lee, Sun Woo Jang, Danbi Park, Chong Man Kim, Jin Hoon Park","doi":"10.14245/ns.2550960.480","DOIUrl":null,"url":null,"abstract":"<p><p>The atlantoaxial (C1-2) junction is among the most technically demanding regions for cervical spine surgery owing to its complex osseoligamentous anatomy and proximity to critical neurovascular structures. Numerous posterior fixation constructs have been developed to optimize biomechanical rigidity and promote arthrodesis. Since Gallie's introduction of posterior wiring with autologous bone grafts in 1939, evolving techniques have focused on enhancing fusion rates while minimizing risk to adjacent structures. This paper outlines the historical evolution of C1-2 posterior instrumentation, current fixation strategies, bone fusion techniques, and reduction methods. A systematic literature search identified 61 relevant studies on C1-2 fusion. Additional references were manually reviewed to provide a comprehensive context. Of these, 41 studies were narratively summarized to outline the historical and conceptual evolution of C1-2 fusion techniques, while the remaining 20 post-2000 studies on contemporary surgical modifications were systematically reviewed and tabulated for technical details and clinical outcomes. C1-2 fusion techniques have evolved significantly over time. Early methods primarily involved posterior wiring with autologous bone grafts, but later transitioned to rigid segmental fixation using pedicle screw constructs, resulting in improved fusion rates and clinical outcomes. Interarticular fusion, when concurrently performed, enhances the biological fusion environment, contributing to favorable clinical results. C1 lateral mass, posterior arch, pedicle screws and C2 pedicle, lamina screws give us much stronger stability and higher fusion rates. Interarticular fusion using local bone also gives us technical easiness guaranteeing high fusion rate overcoming inconvenience of wiring and iliac bone harvest. Interarticular height reduction and interarticular fusion should be discriminated.</p>","PeriodicalId":19269,"journal":{"name":"Neurospine","volume":"22 3","pages":"634-649"},"PeriodicalIF":3.6000,"publicationDate":"2025-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12518907/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Neurospine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.14245/ns.2550960.480","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/9/30 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
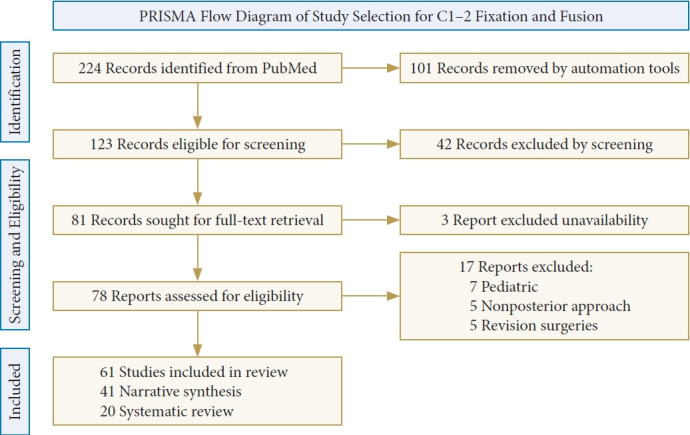
The atlantoaxial (C1-2) junction is among the most technically demanding regions for cervical spine surgery owing to its complex osseoligamentous anatomy and proximity to critical neurovascular structures. Numerous posterior fixation constructs have been developed to optimize biomechanical rigidity and promote arthrodesis. Since Gallie's introduction of posterior wiring with autologous bone grafts in 1939, evolving techniques have focused on enhancing fusion rates while minimizing risk to adjacent structures. This paper outlines the historical evolution of C1-2 posterior instrumentation, current fixation strategies, bone fusion techniques, and reduction methods. A systematic literature search identified 61 relevant studies on C1-2 fusion. Additional references were manually reviewed to provide a comprehensive context. Of these, 41 studies were narratively summarized to outline the historical and conceptual evolution of C1-2 fusion techniques, while the remaining 20 post-2000 studies on contemporary surgical modifications were systematically reviewed and tabulated for technical details and clinical outcomes. C1-2 fusion techniques have evolved significantly over time. Early methods primarily involved posterior wiring with autologous bone grafts, but later transitioned to rigid segmental fixation using pedicle screw constructs, resulting in improved fusion rates and clinical outcomes. Interarticular fusion, when concurrently performed, enhances the biological fusion environment, contributing to favorable clinical results. C1 lateral mass, posterior arch, pedicle screws and C2 pedicle, lamina screws give us much stronger stability and higher fusion rates. Interarticular fusion using local bone also gives us technical easiness guaranteeing high fusion rate overcoming inconvenience of wiring and iliac bone harvest. Interarticular height reduction and interarticular fusion should be discriminated.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


