{"title":"Improving neonatal total parenteral nutrition (TPN) safety and standardisation in a tertiary NICU: a multicomponent QI initiative.","authors":"Priyadarshini Virupaxi Chougula, Pardha Ramineni, Vikrant Rajendra Deshmukh, Pradeep Suryawanshi, Suprabha Kumari Patnaik","doi":"10.1136/bmjpo-2025-003851","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Total parenteral nutrition (TPN) is essential for newborns admitted to the neonatal intensive care unit (NICU) who are unable to meet their nutritional requirements through enteral feeding. However, practices often vary due to resource constraints, lack of standardisation and inadequate training-leading to contamination risks, suboptimal nutrition and increased infections. At our 60-bed tertiary NICU (≈1500 admissions/year), adherence to TPN standards was only 10%. This quality improvement project aimed to increase adherence to >80% through a structured, multidisciplinary protocol.</p><p><strong>Methods: </strong>A stepwise quality improvement initiative using planning, implementation, evaluation and action cycles was implemented. Interventions included shifting TPN preparation to trained residents, introducing a laminar flow surveillance system, deploying an Excel-based TPN calculator, modifying TPN composition to reduce contamination and establishing a rotation schedule. Ongoing training, competency checks and real-time monitoring were incorporated to support sustainability.</p><p><strong>Results: </strong>Adherence to standardised TPN practices improved from a baseline of ~10% to sustained levels, with an overall mean adherence of 84.2% . The Statistical Process Control (SPC) analysis demonstrated a centreline shift from 66.0% in the early unstable phase to 94.1% in the stable phase, confirming sustained process improvement. As a balancing outcome, the overall sepsis incidence among inborn neonates on TPN was 3.2%.</p><p><strong>Conclusion: </strong>This quality improvement initiative successfully enhanced adherence to standardised TPN protocols in the NICU through structured training, workflow optimisation and process surveillance. The structured, practical and team-based approach offers a scalable model for improving the quality and consistency of TPN practices in resource-limited settings, with sustained monitoring and regular training remaining essential for long-term success.</p>","PeriodicalId":9069,"journal":{"name":"BMJ Paediatrics Open","volume":"9 1","pages":""},"PeriodicalIF":2.3000,"publicationDate":"2025-10-07","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12506097/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMJ Paediatrics Open","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1136/bmjpo-2025-003851","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"PEDIATRICS","Score":null,"Total":0}
引用次数: 0
Abstract
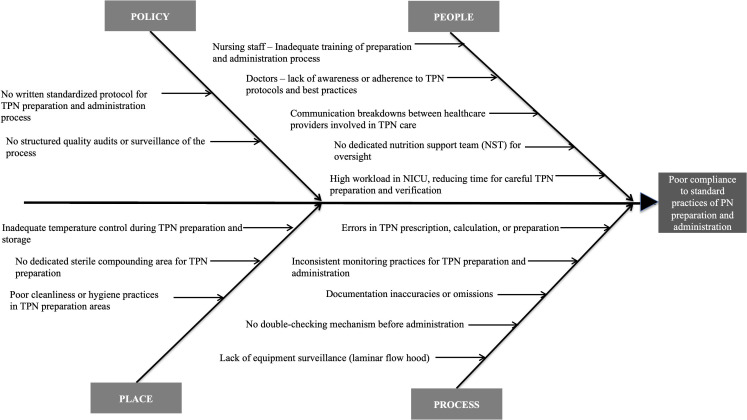
Introduction: Total parenteral nutrition (TPN) is essential for newborns admitted to the neonatal intensive care unit (NICU) who are unable to meet their nutritional requirements through enteral feeding. However, practices often vary due to resource constraints, lack of standardisation and inadequate training-leading to contamination risks, suboptimal nutrition and increased infections. At our 60-bed tertiary NICU (≈1500 admissions/year), adherence to TPN standards was only 10%. This quality improvement project aimed to increase adherence to >80% through a structured, multidisciplinary protocol.
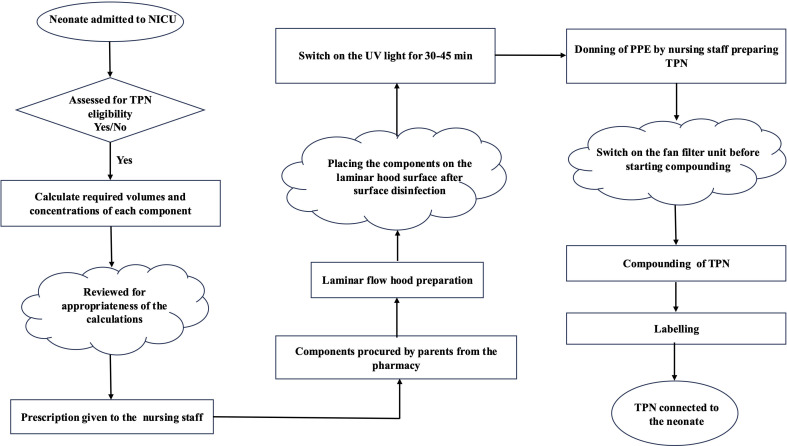
Methods: A stepwise quality improvement initiative using planning, implementation, evaluation and action cycles was implemented. Interventions included shifting TPN preparation to trained residents, introducing a laminar flow surveillance system, deploying an Excel-based TPN calculator, modifying TPN composition to reduce contamination and establishing a rotation schedule. Ongoing training, competency checks and real-time monitoring were incorporated to support sustainability.
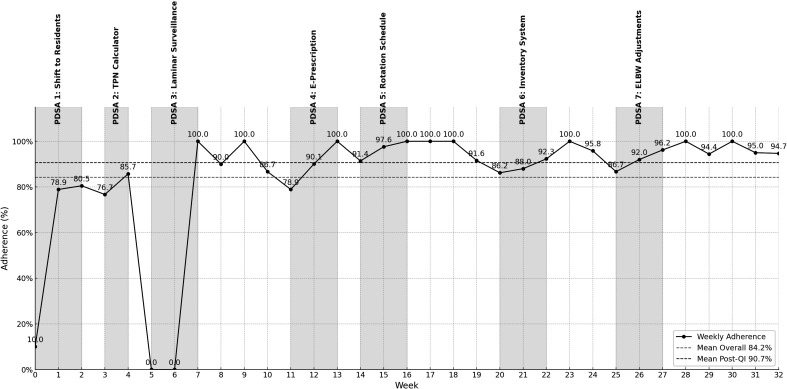
Results: Adherence to standardised TPN practices improved from a baseline of ~10% to sustained levels, with an overall mean adherence of 84.2% . The Statistical Process Control (SPC) analysis demonstrated a centreline shift from 66.0% in the early unstable phase to 94.1% in the stable phase, confirming sustained process improvement. As a balancing outcome, the overall sepsis incidence among inborn neonates on TPN was 3.2%.
Conclusion: This quality improvement initiative successfully enhanced adherence to standardised TPN protocols in the NICU through structured training, workflow optimisation and process surveillance. The structured, practical and team-based approach offers a scalable model for improving the quality and consistency of TPN practices in resource-limited settings, with sustained monitoring and regular training remaining essential for long-term success.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


