Guoxing Tang, Huijuan Song, Liyan Mao, Shaozhen Yan, Lei Tian, Cui Jian, Zhongju Chen, Ziyong Sun, Yue Wang
{"title":"Risk Factor Analysis of CRE Infections at Different Anatomical Sites in ICU Patients.","authors":"Guoxing Tang, Huijuan Song, Liyan Mao, Shaozhen Yan, Lei Tian, Cui Jian, Zhongju Chen, Ziyong Sun, Yue Wang","doi":"10.3390/antibiotics14090884","DOIUrl":null,"url":null,"abstract":"<p><p><b>Objectives</b>: This study aimed to identify differences in risk factors for carbapenem-resistant Enterobacteriaceae (CRE) infections across different anatomical sites and to explore risk factors associated with mortality in CRE-infected patients. <b>Methods</b>: Patients who underwent CRE screening and were subsequently diagnosed with CRE infections were included and categorized by infection site: respiratory tract (RTI), urinary tract (UTI), and bloodstream (BSI). Forty ICU patients without CRE infection were randomly selected as controls. Statistical comparisons were performed using the Mann-Whitney U or Chi-square test, as appropriate. Potential risk factors were evaluated via univariate and multivariate analyses, and a predictive model was constructed, with its performance assessed using ROC curve analysis. <b>Results</b>: CRE colonization was identified as a common independent risk factor across all three groups (RTI, UTI, and BSI). Infection-site-specific analyses revealed independent risk factors: RTI was associated with mechanical ventilation, UTI with trauma, and BSI with gastrointestinal injury. Predictive models for RTI, UTI, and BSI demonstrated good discrimination, with ROC AUCs of 0.94, 0.94, and 0.95, respectively. In the analysis of Survived versus Deceased patients, the BSI group had the highest mortality, though the difference was not statistically significant. Deceased patients exhibited significantly higher PCT levels than Survived patients (<i>p</i> = 0.005). Prior use of carbapenems and antifungal agents, as well as Ln(PCT), were independently associated with mortality in CRE-infected patients. <b>Conclusions</b>: Risk factors for CRE infections vary across anatomical sites, with CRE colonization, mechanical ventilation, trauma, and gastrointestinal injury playing key roles. Overuse of antibiotics and elevated inflammatory responses are associated with increased mortality. These findings provide evidence for early identification of high-risk patients and optimization of individualized treatment strategies.</p>","PeriodicalId":54246,"journal":{"name":"Antibiotics-Basel","volume":"14 9","pages":""},"PeriodicalIF":4.6000,"publicationDate":"2025-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12466705/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Antibiotics-Basel","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.3390/antibiotics14090884","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"INFECTIOUS DISEASES","Score":null,"Total":0}
引用次数: 0
Abstract
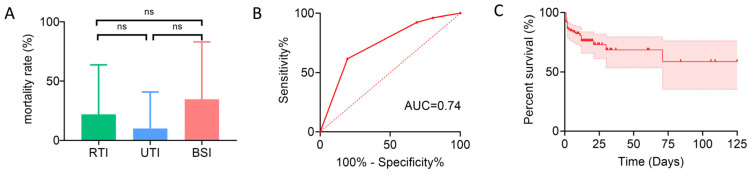
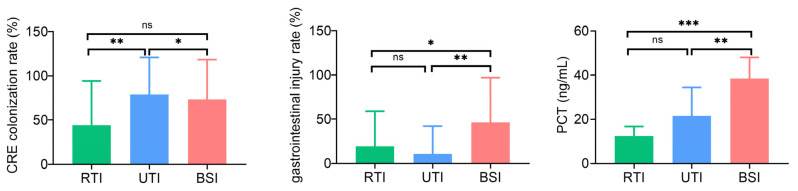
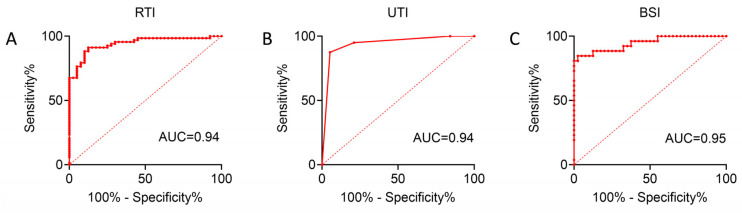
Objectives: This study aimed to identify differences in risk factors for carbapenem-resistant Enterobacteriaceae (CRE) infections across different anatomical sites and to explore risk factors associated with mortality in CRE-infected patients. Methods: Patients who underwent CRE screening and were subsequently diagnosed with CRE infections were included and categorized by infection site: respiratory tract (RTI), urinary tract (UTI), and bloodstream (BSI). Forty ICU patients without CRE infection were randomly selected as controls. Statistical comparisons were performed using the Mann-Whitney U or Chi-square test, as appropriate. Potential risk factors were evaluated via univariate and multivariate analyses, and a predictive model was constructed, with its performance assessed using ROC curve analysis. Results: CRE colonization was identified as a common independent risk factor across all three groups (RTI, UTI, and BSI). Infection-site-specific analyses revealed independent risk factors: RTI was associated with mechanical ventilation, UTI with trauma, and BSI with gastrointestinal injury. Predictive models for RTI, UTI, and BSI demonstrated good discrimination, with ROC AUCs of 0.94, 0.94, and 0.95, respectively. In the analysis of Survived versus Deceased patients, the BSI group had the highest mortality, though the difference was not statistically significant. Deceased patients exhibited significantly higher PCT levels than Survived patients (p = 0.005). Prior use of carbapenems and antifungal agents, as well as Ln(PCT), were independently associated with mortality in CRE-infected patients. Conclusions: Risk factors for CRE infections vary across anatomical sites, with CRE colonization, mechanical ventilation, trauma, and gastrointestinal injury playing key roles. Overuse of antibiotics and elevated inflammatory responses are associated with increased mortality. These findings provide evidence for early identification of high-risk patients and optimization of individualized treatment strategies.
Antibiotics-BaselPharmacology, Toxicology and Pharmaceutics-General Pharmacology, Toxicology and Pharmaceutics
CiteScore
7.30
自引率
14.60%
发文量
1547
审稿时长
11 weeks
期刊介绍:
Antibiotics (ISSN 2079-6382) is an open access, peer reviewed journal on all aspects of antibiotics. Antibiotics is a multi-disciplinary journal encompassing the general fields of biochemistry, chemistry, genetics, microbiology and pharmacology. Our aim is to encourage scientists to publish their experimental and theoretical results in as much detail as possible. Therefore, there is no restriction on the length of papers.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


