{"title":"Accrual of thromboembolic events and antiphospholipid syndrome in new-onset systemic lupus erythematosus: a population-based inception cohort study.","authors":"Sigrid Reppe Moe, Hilde Haukeland, Cathrine Brunborg, Antonela Botea, Nenad Damjanic, Gro Årthun Wivestad, Heidi Kverneggen Øvreås, Thea Bjerkestrand Bøe, Anniken Orre, Garen Torhild, Sella Aarrestad Provan, Øyvind Molberg, Karoline Lerang","doi":"10.1136/rmdopen-2025-005795","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>This population-based study aimed to determine timing and incidence of arterial and venous thromboembolic events (TE) and antiphospholipid syndrome (APS) relative to systemic lupus erythematosus (SLE) onset and assess relationships between TE, APS and anti-phospholipid antibodies (aPL) during follow-up.</p><p><strong>Methods: </strong>We included all medical-record confirmed new-onset SLE patients in Southeast Norway (population 2.9 million) 2000-2017 who fulfilled the 2019 European Alliance of Rheumatology Associations/American College of Rheumatology classification criteria. APS was defined by the 2006 Sydney classification criteria, and aPL positivity was determined following international guidelines. Key outcomes were APS, TE and death. We estimated outcome-free survival using Kaplan-Meier methods.</p><p><strong>Results: </strong>Among 700 new-onset SLE patients followed for a mean of 8 years (SD 5.0), 13% (89/700) experienced a new TE. TE incidence peaked at 59 per 100 person-years (95% CI 38 to 87) in the first year of SLE among aPL positive patients diagnosed with APS, falling to 12 (95% CI 6.2 to 21) in the subsequent 4 years. In patients without APS, corresponding TE incidences were 2.6 (95% CI 1.4 to 4.3) and 0.9 (95% CI 0.5 to 1.4), respectively. The lowest TE incidence was in aPL-negative patients aged <50 years, with 1-year TE-free survival of 0.99 (95% CI 0.97 to 1.0). Beyond the first year, TE-free survival rates did not differ between SLE patients positive and negative for aPL. Standardised mortality rate in patients with and without APS was 4.7 (95% CI 1.8 to 10.7 and 1.7 (95% CI 1.2 to 2.3).</p><p><strong>Conclusions: </strong>This population-level study reveals high risk of TE, particularly for aPL positive patients around the time of SLE diagnosis. The elevated TE risk requires attention and early preventive strategies in newly diagnosed SLE.</p>","PeriodicalId":21396,"journal":{"name":"RMD Open","volume":"11 3","pages":""},"PeriodicalIF":4.7000,"publicationDate":"2025-09-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12406804/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"RMD Open","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1136/rmdopen-2025-005795","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"RHEUMATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: This population-based study aimed to determine timing and incidence of arterial and venous thromboembolic events (TE) and antiphospholipid syndrome (APS) relative to systemic lupus erythematosus (SLE) onset and assess relationships between TE, APS and anti-phospholipid antibodies (aPL) during follow-up.
Methods: We included all medical-record confirmed new-onset SLE patients in Southeast Norway (population 2.9 million) 2000-2017 who fulfilled the 2019 European Alliance of Rheumatology Associations/American College of Rheumatology classification criteria. APS was defined by the 2006 Sydney classification criteria, and aPL positivity was determined following international guidelines. Key outcomes were APS, TE and death. We estimated outcome-free survival using Kaplan-Meier methods.
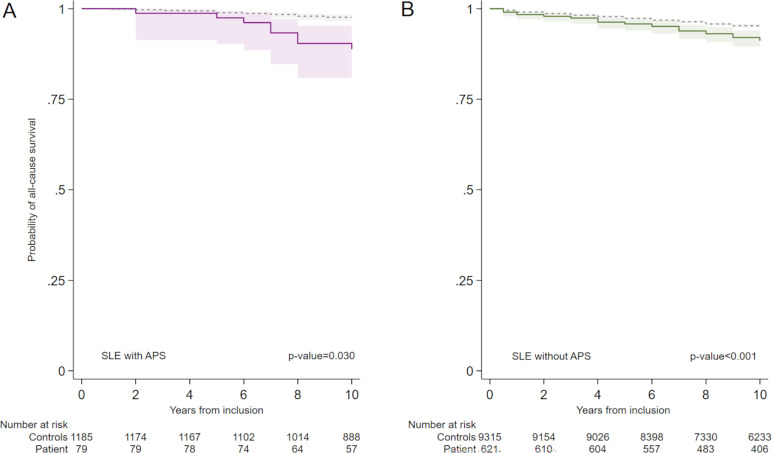
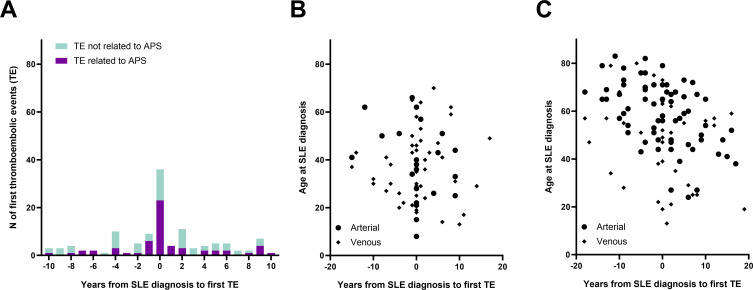
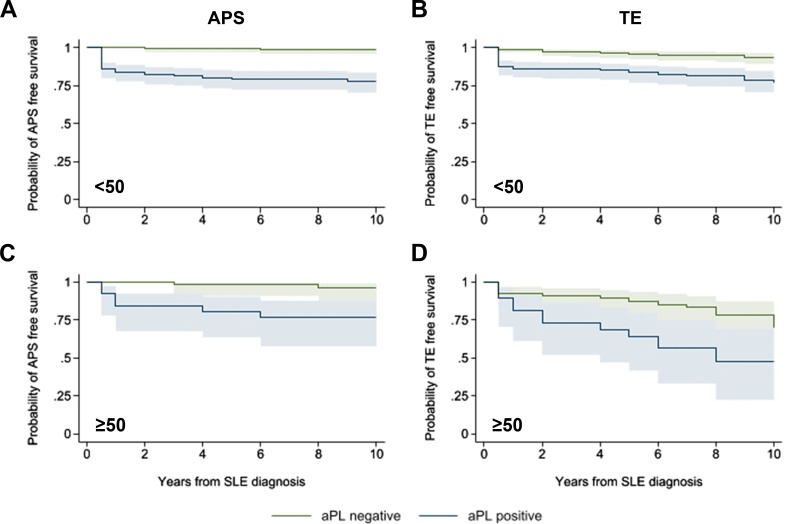
Results: Among 700 new-onset SLE patients followed for a mean of 8 years (SD 5.0), 13% (89/700) experienced a new TE. TE incidence peaked at 59 per 100 person-years (95% CI 38 to 87) in the first year of SLE among aPL positive patients diagnosed with APS, falling to 12 (95% CI 6.2 to 21) in the subsequent 4 years. In patients without APS, corresponding TE incidences were 2.6 (95% CI 1.4 to 4.3) and 0.9 (95% CI 0.5 to 1.4), respectively. The lowest TE incidence was in aPL-negative patients aged <50 years, with 1-year TE-free survival of 0.99 (95% CI 0.97 to 1.0). Beyond the first year, TE-free survival rates did not differ between SLE patients positive and negative for aPL. Standardised mortality rate in patients with and without APS was 4.7 (95% CI 1.8 to 10.7 and 1.7 (95% CI 1.2 to 2.3).
Conclusions: This population-level study reveals high risk of TE, particularly for aPL positive patients around the time of SLE diagnosis. The elevated TE risk requires attention and early preventive strategies in newly diagnosed SLE.
期刊介绍:
RMD Open publishes high quality peer-reviewed original research covering the full spectrum of musculoskeletal disorders, rheumatism and connective tissue diseases, including osteoporosis, spine and rehabilitation. Clinical and epidemiological research, basic and translational medicine, interesting clinical cases, and smaller studies that add to the literature are all considered.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


