{"title":"Blastomycosis in a Renal Transplant Recipient: A Rare Encounter in Rural Appalachia.","authors":"Khawaja O Omar, William Sebastian, Suzanne Kemper","doi":"10.55729/2000-9666.1470","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Blastomycosis is a fungal infection caused by <i>Blastomyces</i> species, which are thermally dimorphic fungi endemic to the midwestern, south-central, and southeastern United States (US). Organ transplant patients are at risk of infection due to long-term immunosuppressive therapy. We present a unique case of blastomycosis in a renal transplant patient residing in a non-endemic region of Appalachia.</p><p><strong>Case report: </strong>A 67-year-old patient with history of tobacco use, atrial fibrillation, type 2 diabetes, hyperlipidemia, and bilateral deceased donor kidney transplantation (DDKT) in 2021, presented to Charleston Area Medical Center's (CAMC), Charleston WV, Emergency Department (ED) for fever and night sweats. Initial workup revealed 39.4 °C temperature with remaining vital signs normal. Corona, parainfluenza, influenza, metapneumovirus, mycoplasma pneumonia, RSV were negative, GI PCR panel was negative for C. difficle, yersinia, campylobacter, giardia, vibrio, norovirus, salmonella, rotavirus. Chest X-ray showed a 2.1 × 1.6 cm nodular density in the left upper lobe (LUL) lobe. White blood cell (WBC) count was elevated at 13000/mcl with a left-sided shift. Subsequent computed tomography (CT) of the chest without contrast demonstrated a 2.7 × 2.1 cm LUL mass. Urine <i>Blastomyces</i> antigen tested positive, prompting the initiation of empiric therapy for blastomycosis. Aspergillus was ruled out initially.</p><p><strong>Conclusion: </strong>Blastomycosis is a rare occurrence in the US, with annual incidence reported at 1 to 2 cases per 100,000. While transplant recipients are predisposed to acquiring blastomycosis, it remains an infrequent occurrence. In transplant patients presenting with persistent infectious symptoms, blastomycosis and other rare etiologies should be considered to prevent severe complications.</p>","PeriodicalId":15460,"journal":{"name":"Journal of Community Hospital Internal Medicine Perspectives","volume":"15 4","pages":"96-99"},"PeriodicalIF":0.6000,"publicationDate":"2025-07-03","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12315875/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Community Hospital Internal Medicine Perspectives","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.55729/2000-9666.1470","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Blastomycosis is a fungal infection caused by Blastomyces species, which are thermally dimorphic fungi endemic to the midwestern, south-central, and southeastern United States (US). Organ transplant patients are at risk of infection due to long-term immunosuppressive therapy. We present a unique case of blastomycosis in a renal transplant patient residing in a non-endemic region of Appalachia.
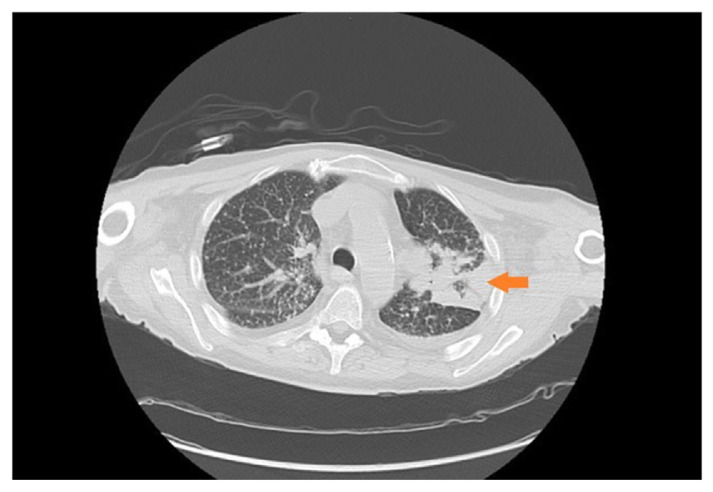
Case report: A 67-year-old patient with history of tobacco use, atrial fibrillation, type 2 diabetes, hyperlipidemia, and bilateral deceased donor kidney transplantation (DDKT) in 2021, presented to Charleston Area Medical Center's (CAMC), Charleston WV, Emergency Department (ED) for fever and night sweats. Initial workup revealed 39.4 °C temperature with remaining vital signs normal. Corona, parainfluenza, influenza, metapneumovirus, mycoplasma pneumonia, RSV were negative, GI PCR panel was negative for C. difficle, yersinia, campylobacter, giardia, vibrio, norovirus, salmonella, rotavirus. Chest X-ray showed a 2.1 × 1.6 cm nodular density in the left upper lobe (LUL) lobe. White blood cell (WBC) count was elevated at 13000/mcl with a left-sided shift. Subsequent computed tomography (CT) of the chest without contrast demonstrated a 2.7 × 2.1 cm LUL mass. Urine Blastomyces antigen tested positive, prompting the initiation of empiric therapy for blastomycosis. Aspergillus was ruled out initially.
Conclusion: Blastomycosis is a rare occurrence in the US, with annual incidence reported at 1 to 2 cases per 100,000. While transplant recipients are predisposed to acquiring blastomycosis, it remains an infrequent occurrence. In transplant patients presenting with persistent infectious symptoms, blastomycosis and other rare etiologies should be considered to prevent severe complications.
期刊介绍:
JCHIMP provides: up-to-date information in the field of Internal Medicine to community hospital medical professionals a platform for clinical faculty, residents, and medical students to publish research relevant to community hospital programs. Manuscripts that explore aspects of medicine at community hospitals welcome, including but not limited to: the best practices of community academic programs community hospital-based research opinion and insight from community hospital leadership and faculty the scholarly work of residents and medical students affiliated with community hospitals.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


