Franz Felix Konen, Torsten Witte, Diana Ernst, David Hagin, Konstantin Fritz Jendretzky, Nora Möhn, Sandra Nay, Lea Grote-Levi, Kurt-Wolfram Sühs, Luisa Klotz, Steffen Pfeuffer, Refik Pul, Christoph Kleinschnitz, Marc Pawlitzki, Sven G Meuth, Thomas Skripuletz
{"title":"Management of disease-modifying therapies in multiple sclerosis and comorbid rheumatoid arthritis.","authors":"Franz Felix Konen, Torsten Witte, Diana Ernst, David Hagin, Konstantin Fritz Jendretzky, Nora Möhn, Sandra Nay, Lea Grote-Levi, Kurt-Wolfram Sühs, Luisa Klotz, Steffen Pfeuffer, Refik Pul, Christoph Kleinschnitz, Marc Pawlitzki, Sven G Meuth, Thomas Skripuletz","doi":"10.1186/s42466-025-00414-y","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Comorbid autoimmune disorders, including rheumatoid arthritis (RA), are common in people with multiple sclerosis (MS). Both conditions share pathogenic similarities, enabling potential overlap in treatments. While numerous disease-modifying therapies (DMT) are approved for MS and new options are under clinical trial, their effectiveness in RA varies.</p><p><strong>Main body: </strong>A PubMed literature review was conducted to evaluate the effects of approved and currently investigated MS-DMT on MS and RA and vice versa. Certain MS-DMT showed beneficial effects for RA, such as teriflunomide, anti-CD20 therapies, and cladribine, while others demonstrated no significant impact (type-I interferons, Bruton´s tyrosine kinase (BTK) inhibitors) or lacked trials (sphingosine-1-phosphate receptor modulators, glatiramer acetate). In contrast, BTK inhibitors were shown to be effective for inactive secondary progressive forms of MS, whereas secukinumab showed limited effects in relapsing MS. Concerning DMT for RA in MS, no significant benefit was observed for abatacept, and there are no trials for Janus kinase inhibitors, or interleukin-(IL)-6 receptor inhibitors (tocilizumab, sarilumab). Adverse events, including RA exacerbation, were reported for some MS-DMT like dimethyl fumarate, alemtuzumab, and natalizumab. Tumor necrosis factor alpha (TNFα) inhibitors increased disease activity in MS patients.</p><p><strong>Conclusion: </strong>Among approved DMT for MS and RA, teriflunomide and anti-CD20 therapies are the most suitable options for moderately or highly active MS with comorbid RA. Cladribine may also be considered, while TNFα inhibitors are contraindicated.</p>","PeriodicalId":94156,"journal":{"name":"Neurological research and practice","volume":"7 1","pages":"48"},"PeriodicalIF":3.2000,"publicationDate":"2025-07-17","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12273305/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Neurological research and practice","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s42466-025-00414-y","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Comorbid autoimmune disorders, including rheumatoid arthritis (RA), are common in people with multiple sclerosis (MS). Both conditions share pathogenic similarities, enabling potential overlap in treatments. While numerous disease-modifying therapies (DMT) are approved for MS and new options are under clinical trial, their effectiveness in RA varies.
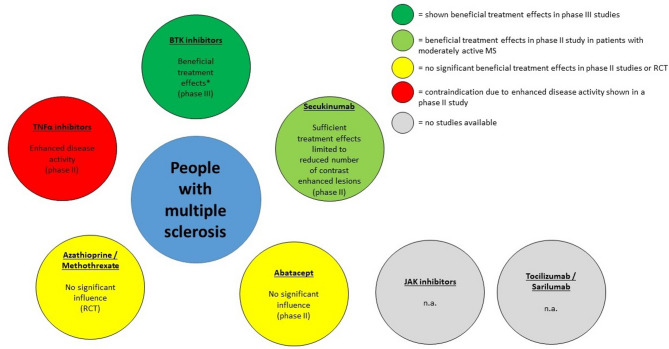
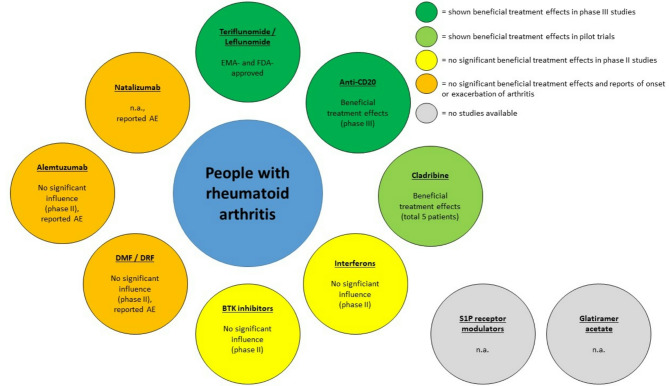
Main body: A PubMed literature review was conducted to evaluate the effects of approved and currently investigated MS-DMT on MS and RA and vice versa. Certain MS-DMT showed beneficial effects for RA, such as teriflunomide, anti-CD20 therapies, and cladribine, while others demonstrated no significant impact (type-I interferons, Bruton´s tyrosine kinase (BTK) inhibitors) or lacked trials (sphingosine-1-phosphate receptor modulators, glatiramer acetate). In contrast, BTK inhibitors were shown to be effective for inactive secondary progressive forms of MS, whereas secukinumab showed limited effects in relapsing MS. Concerning DMT for RA in MS, no significant benefit was observed for abatacept, and there are no trials for Janus kinase inhibitors, or interleukin-(IL)-6 receptor inhibitors (tocilizumab, sarilumab). Adverse events, including RA exacerbation, were reported for some MS-DMT like dimethyl fumarate, alemtuzumab, and natalizumab. Tumor necrosis factor alpha (TNFα) inhibitors increased disease activity in MS patients.
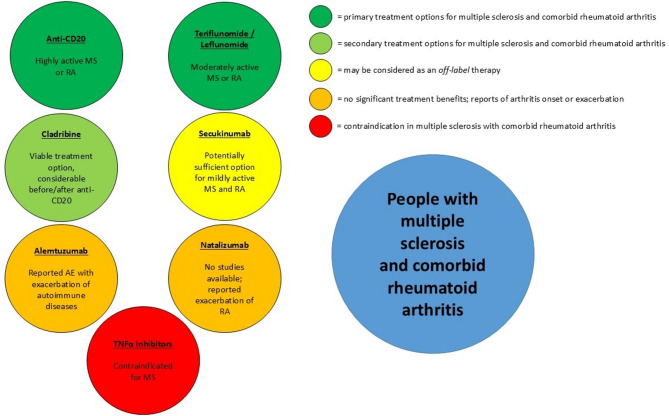
Conclusion: Among approved DMT for MS and RA, teriflunomide and anti-CD20 therapies are the most suitable options for moderately or highly active MS with comorbid RA. Cladribine may also be considered, while TNFα inhibitors are contraindicated.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


