Machine learning approaches to identify neonates and young children at risk for postdischarge mortality in Dar es Salaam, Tanzania and Monrovia, Liberia.
Chris A Rees, Rodrick Kisenge, Evance Godfrey, Readon C Ideh, Julia Kamara, Ye-Jeung G Coleman-Nekar, Abraham Samma, Hussein K Manji, Christopher R Sudfeld, Adrianna L Westbrook, Michelle Niescierenko, Claudia R Morris, Todd A Florin, Cynthia G Whitney, Karim P Manji, Christopher P Duggan, Rishikesan Kamaleswaran
{"title":"Machine learning approaches to identify neonates and young children at risk for postdischarge mortality in Dar es Salaam, Tanzania and Monrovia, Liberia.","authors":"Chris A Rees, Rodrick Kisenge, Evance Godfrey, Readon C Ideh, Julia Kamara, Ye-Jeung G Coleman-Nekar, Abraham Samma, Hussein K Manji, Christopher R Sudfeld, Adrianna L Westbrook, Michelle Niescierenko, Claudia R Morris, Todd A Florin, Cynthia G Whitney, Karim P Manji, Christopher P Duggan, Rishikesan Kamaleswaran","doi":"10.1136/bmjpo-2025-003547","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The time after hospital discharge carries high rates of mortality in neonates and young children in sub-Saharan Africa. Previous work using logistic regression to develop risk assessment tools to identify those at risk for postdischarge mortality has yielded fair discriminatory value. Our objective was to determine if machine learning models would have greater discriminatory value to identify neonates and young children at risk for postdischarge mortality.</p><p><strong>Methods: </strong>We conducted a planned secondary analysis of a prospective observational cohort at Muhimbili National Hospital in Dar es Salaam, Tanzania and John F. Kennedy Medical Center in Monrovia, Liberia. We enrolled neonates and young children near the time of discharge. The outcome was 60-day postdischarge mortality. We collected socioeconomic, demographic, clinical, and anthropometric data during hospital admission and used machine learning (ie, eXtreme Gradient Boosting (XGBoost), Hist-Gradient Boost, Support Vector Machine, Neural Network, and Random Forest) to develop risk assessment tools to identify: (1) neonates and (2) young children at risk for postdischarge mortality.</p><p><strong>Results: </strong>A total of 2310 neonates and 1933 young children enrolled. Of these, 71 (3.1%) neonates and 67 (3.5%) young children died after hospital discharge. XGBoost, Hist Gradient Boost, and Neural Network models yielded the greatest discriminatory value (area under the receiver operating characteristic curves range: 0.94-0.99) and fewest features, which included six features for neonates and five for young children. Discharge against medical advice, low birth weight, and supplemental oxygen requirement during hospitalisation were predictive of postdischarge mortality in neonates. For young children, discharge against medical advice, pallor, and chronic medical problems were predictive of postdischarge mortality.</p><p><strong>Conclusions: </strong>Our parsimonious machine learning-based models had excellent discriminatory value to predict postdischarge mortality among neonates and young children. External validation of these tools is warranted to assist in the design of interventions to reduce postdischarge mortality in these vulnerable populations.</p>","PeriodicalId":9069,"journal":{"name":"BMJ Paediatrics Open","volume":"9 1","pages":""},"PeriodicalIF":2.3000,"publicationDate":"2025-06-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12182169/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMJ Paediatrics Open","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1136/bmjpo-2025-003547","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"PEDIATRICS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: The time after hospital discharge carries high rates of mortality in neonates and young children in sub-Saharan Africa. Previous work using logistic regression to develop risk assessment tools to identify those at risk for postdischarge mortality has yielded fair discriminatory value. Our objective was to determine if machine learning models would have greater discriminatory value to identify neonates and young children at risk for postdischarge mortality.
Methods: We conducted a planned secondary analysis of a prospective observational cohort at Muhimbili National Hospital in Dar es Salaam, Tanzania and John F. Kennedy Medical Center in Monrovia, Liberia. We enrolled neonates and young children near the time of discharge. The outcome was 60-day postdischarge mortality. We collected socioeconomic, demographic, clinical, and anthropometric data during hospital admission and used machine learning (ie, eXtreme Gradient Boosting (XGBoost), Hist-Gradient Boost, Support Vector Machine, Neural Network, and Random Forest) to develop risk assessment tools to identify: (1) neonates and (2) young children at risk for postdischarge mortality.
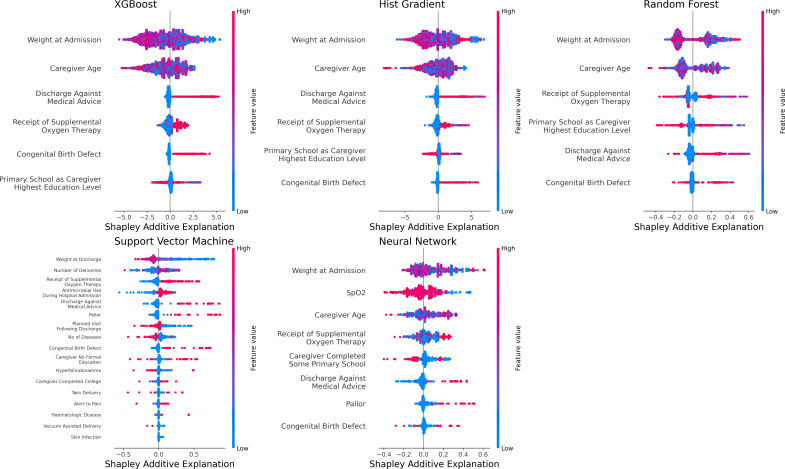
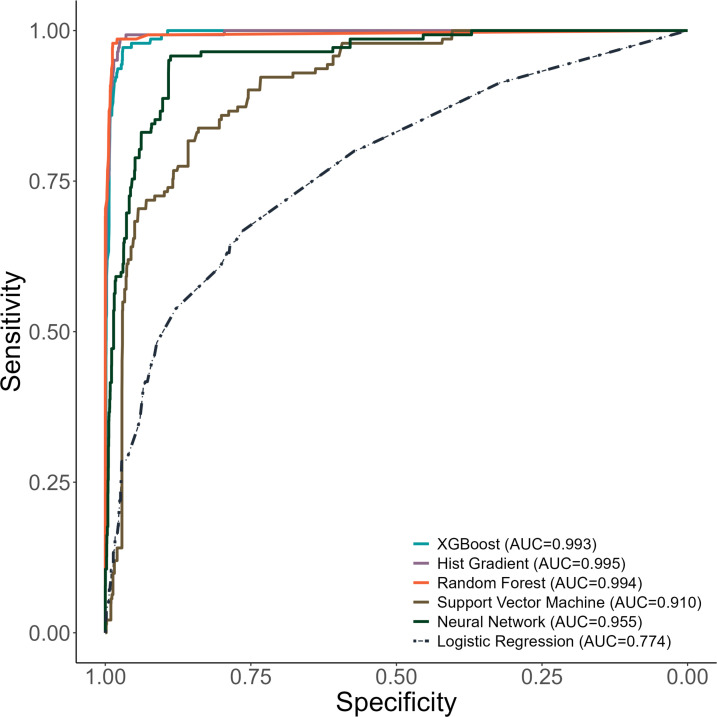
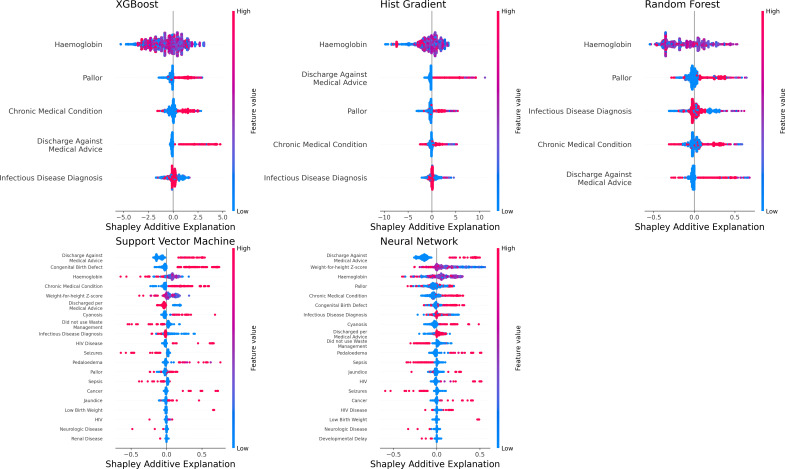
Results: A total of 2310 neonates and 1933 young children enrolled. Of these, 71 (3.1%) neonates and 67 (3.5%) young children died after hospital discharge. XGBoost, Hist Gradient Boost, and Neural Network models yielded the greatest discriminatory value (area under the receiver operating characteristic curves range: 0.94-0.99) and fewest features, which included six features for neonates and five for young children. Discharge against medical advice, low birth weight, and supplemental oxygen requirement during hospitalisation were predictive of postdischarge mortality in neonates. For young children, discharge against medical advice, pallor, and chronic medical problems were predictive of postdischarge mortality.
Conclusions: Our parsimonious machine learning-based models had excellent discriminatory value to predict postdischarge mortality among neonates and young children. External validation of these tools is warranted to assist in the design of interventions to reduce postdischarge mortality in these vulnerable populations.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


