{"title":"Disparities in end-of-life care and place of death in people with malignant brain tumors-A Swedish registry study.","authors":"Anneli Ozanne, Joakim Öhlén, Stina Nyblom, Asgeir Store Jakola, Anja Smits, Cecilia Larsdotter","doi":"10.1093/nop/npae113","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Malignant brain tumors often lead to death. While improving future treatments is essential, end-of-life care must also be addressed. To ensure equitable palliative care, understanding the place of death is crucial, as disparities may lead to inequity of care. This study aims to identify the place of death in adults with malignant brain tumors in Sweden, and the potential associations with official palliative care status by the ICD-10 code Z51.5, sociodemographic factors, health service characteristics, and healthcare service utilization.</p><p><strong>Methods: </strong>A population-level registry study examined the place of death among adults who died of malignant brain tumors in Sweden from 2013 to 2019. Descriptive statistics, univariable, and multivariable binary logistic regression analyses were performed.</p><p><strong>Results: </strong>We identified 3,888 adults who died from malignant brain tumors. Of these, 64.4% did not receive an official palliative care status. Specialized palliative care was not utilized in 57.2% at the place of death and in 80% of nursing home deaths. In the last month of life, 53.5% of hospital deaths involved 1 transfer, while 41.8% had 2 or more transfers. The odds ratio (OR) of dying in hospital versus at home was higher, with 2 or more transfers (OR 0.63 [0.40, 0.99]). The OR of dying in a hospital versus at home showed significant regional differences.</p><p><strong>Conclusions: </strong>Despite the severity of their diagnosis, only a minority of patients utilized specialized palliative services at death, and this varied by the place of death. Significant regional disparities were found between hospital and home deaths, indicating unequal end-of-life palliative care in this patient group.</p>","PeriodicalId":19234,"journal":{"name":"Neuro-oncology practice","volume":"12 3","pages":"511-519"},"PeriodicalIF":2.5000,"publicationDate":"2024-11-11","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12137219/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Neuro-oncology practice","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/nop/npae113","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/6/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Malignant brain tumors often lead to death. While improving future treatments is essential, end-of-life care must also be addressed. To ensure equitable palliative care, understanding the place of death is crucial, as disparities may lead to inequity of care. This study aims to identify the place of death in adults with malignant brain tumors in Sweden, and the potential associations with official palliative care status by the ICD-10 code Z51.5, sociodemographic factors, health service characteristics, and healthcare service utilization.
Methods: A population-level registry study examined the place of death among adults who died of malignant brain tumors in Sweden from 2013 to 2019. Descriptive statistics, univariable, and multivariable binary logistic regression analyses were performed.
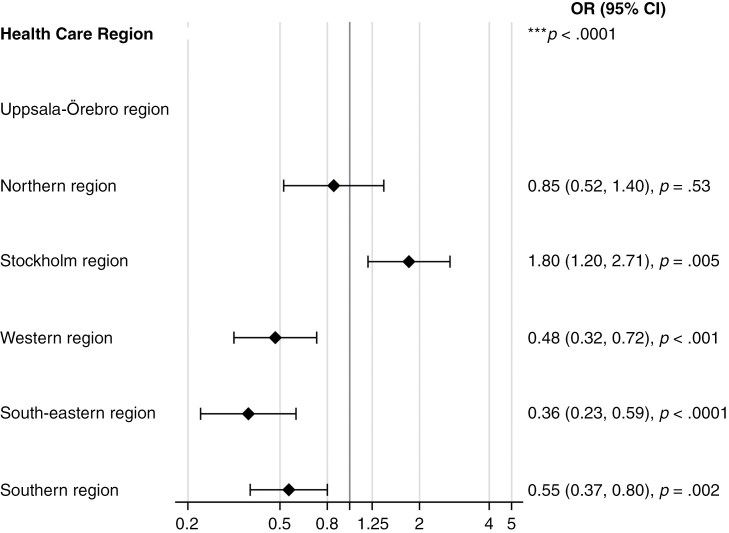
Results: We identified 3,888 adults who died from malignant brain tumors. Of these, 64.4% did not receive an official palliative care status. Specialized palliative care was not utilized in 57.2% at the place of death and in 80% of nursing home deaths. In the last month of life, 53.5% of hospital deaths involved 1 transfer, while 41.8% had 2 or more transfers. The odds ratio (OR) of dying in hospital versus at home was higher, with 2 or more transfers (OR 0.63 [0.40, 0.99]). The OR of dying in a hospital versus at home showed significant regional differences.
Conclusions: Despite the severity of their diagnosis, only a minority of patients utilized specialized palliative services at death, and this varied by the place of death. Significant regional disparities were found between hospital and home deaths, indicating unequal end-of-life palliative care in this patient group.
期刊介绍:
Neuro-Oncology Practice focuses on the clinical aspects of the subspecialty for practicing clinicians and healthcare specialists from a variety of disciplines including physicians, nurses, physical/occupational therapists, neuropsychologists, and palliative care specialists, who have focused their careers on clinical patient care and who want to apply the latest treatment advances to their practice. These include: Applying new trial results to improve standards of patient care Translating scientific advances such as tumor molecular profiling and advanced imaging into clinical treatment decision making and personalized brain tumor therapies Raising awareness of basic, translational and clinical research in areas of symptom management, survivorship, neurocognitive function, end of life issues and caregiving

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


