Tomás Fontes, Alexandre Sepriano, Sofia Ramiro, Paula Moniz, Carolina Furtado, Guilherme Figueiredo, Sandra Falcão
{"title":"Diagnosis of carpal tunnel syndrome with ultrasound: should we go more distal?","authors":"Tomás Fontes, Alexandre Sepriano, Sofia Ramiro, Paula Moniz, Carolina Furtado, Guilherme Figueiredo, Sandra Falcão","doi":"10.1136/rmdopen-2025-005563","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>To assess the value of adding the ultradistal level to other more thoroughly studied levels of the carpal tunnel when measuring the cross-sectional area (CSA) of the median nerve (MN) by ultrasound (US) in diagnosing patients with primary carpal tunnel syndrome (CTS).</p><p><strong>Methods: </strong>Patients clinically diagnosed with primary CTS and healthy controls were included. The MN-CSA was measured by US at three wrist levels: proximal, distal and ultradistal. The best cut-off to differentiate cases and controls was determined for the CSA and for the difference between levels of the same wrist. The performance of different definitions for US-CTS compared with the clinical diagnosis of CTS was evaluated: (1) CSA above cut-off at each level; (2) CSA-difference above cut-off at each level; (3) ≥1 level with CSA above cut-off and (4) ≥1 CSA-difference above cut-off. Definition 3, excluding the ultradistal level, and combinations of definitions were also tested.</p><p><strong>Results: </strong>In total, 219 patients and 39 controls were included. The CSA was higher in patients (10.5-16.8 mm<sup>2</sup>) than controls (6.2-7.6 mm<sup>2</sup>). The difference between groups was maximal at the ultradistal level (right: 10.1 mm<sup>2</sup>; left: 8.3 mm<sup>2</sup>). The CSA cut-offs were 11 mm<sup>2</sup>, 9 mm<sup>2</sup> and 10 mm<sup>2</sup> at the right, and 10 mm<sup>2</sup>, 8 mm<sup>2</sup> and 10 mm<sup>2</sup> at the left, for the proximal, distal and ultradistal levels, respectively. Definition 3 yielded the best balance between sensitivity (98%) and specificity (95%) (right hand). Removing the ultradistal level from definition 3 decreased sensitivity to 90%, maintaining the same specificity.</p><p><strong>Conclusions: </strong>Adding the ultradistal level improves the performance of US for diagnosing CTS. We suggest adding it in clinical practice when investigating CTS.</p>","PeriodicalId":21396,"journal":{"name":"RMD Open","volume":"11 2","pages":""},"PeriodicalIF":4.7000,"publicationDate":"2025-05-28","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12121607/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"RMD Open","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1136/rmdopen-2025-005563","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"RHEUMATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Objectives: To assess the value of adding the ultradistal level to other more thoroughly studied levels of the carpal tunnel when measuring the cross-sectional area (CSA) of the median nerve (MN) by ultrasound (US) in diagnosing patients with primary carpal tunnel syndrome (CTS).
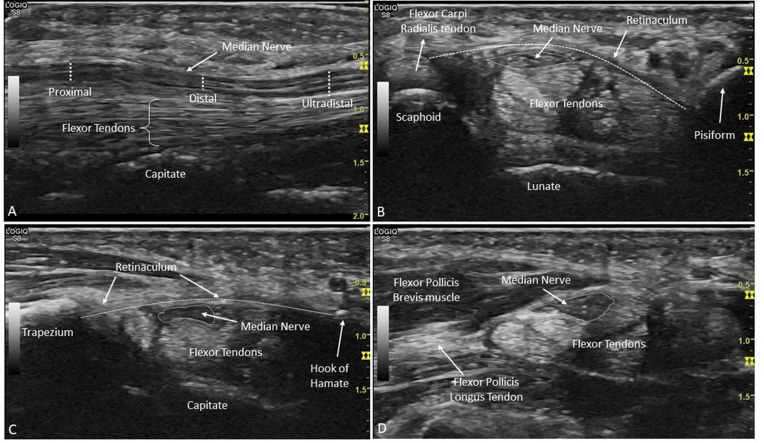
Methods: Patients clinically diagnosed with primary CTS and healthy controls were included. The MN-CSA was measured by US at three wrist levels: proximal, distal and ultradistal. The best cut-off to differentiate cases and controls was determined for the CSA and for the difference between levels of the same wrist. The performance of different definitions for US-CTS compared with the clinical diagnosis of CTS was evaluated: (1) CSA above cut-off at each level; (2) CSA-difference above cut-off at each level; (3) ≥1 level with CSA above cut-off and (4) ≥1 CSA-difference above cut-off. Definition 3, excluding the ultradistal level, and combinations of definitions were also tested.
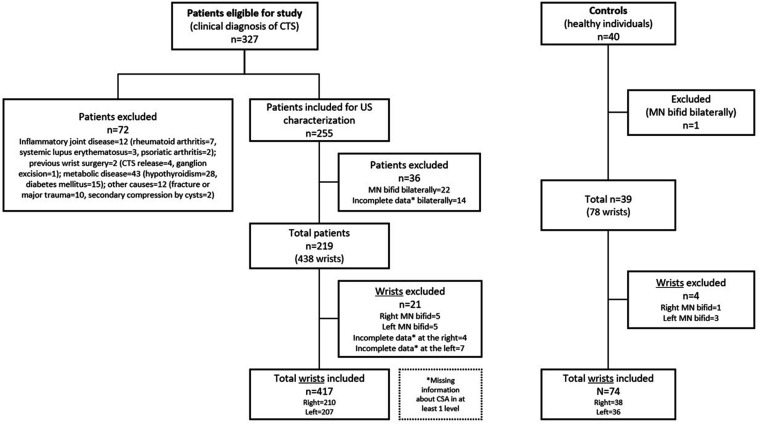
Results: In total, 219 patients and 39 controls were included. The CSA was higher in patients (10.5-16.8 mm2) than controls (6.2-7.6 mm2). The difference between groups was maximal at the ultradistal level (right: 10.1 mm2; left: 8.3 mm2). The CSA cut-offs were 11 mm2, 9 mm2 and 10 mm2 at the right, and 10 mm2, 8 mm2 and 10 mm2 at the left, for the proximal, distal and ultradistal levels, respectively. Definition 3 yielded the best balance between sensitivity (98%) and specificity (95%) (right hand). Removing the ultradistal level from definition 3 decreased sensitivity to 90%, maintaining the same specificity.
Conclusions: Adding the ultradistal level improves the performance of US for diagnosing CTS. We suggest adding it in clinical practice when investigating CTS.
期刊介绍:
RMD Open publishes high quality peer-reviewed original research covering the full spectrum of musculoskeletal disorders, rheumatism and connective tissue diseases, including osteoporosis, spine and rehabilitation. Clinical and epidemiological research, basic and translational medicine, interesting clinical cases, and smaller studies that add to the literature are all considered.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


