Endoscopic Decompression Combined With Percutaneous Pedicle Screw Fixation for AOSpine A3 or A4 Thoracolumbar Fractures With Neurological Deficits: A Retrospective Cohort Study.
{"title":"Endoscopic Decompression Combined With Percutaneous Pedicle Screw Fixation for AOSpine A3 or A4 Thoracolumbar Fractures With Neurological Deficits: A Retrospective Cohort Study.","authors":"Huiming Yang, Junxian Miao, Jiangtao Wang, Dan Han, Yuhang Wang, Liang Yan, Biao Wang, Dingjun Hao","doi":"10.14245/ns.2449212.606","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>This study aimed to compare the clinical outcomes of patients with AOSpine A3 or A4 thoracolumbar fractures presenting with neurological deficits treated with endoscopic decompression combined with percutaneous pedicle screws fixation (endoscopic minimally invasive surgery, EMIS) or conventional open surgery (OS).</p><p><strong>Methods: </strong>Data of patients with AOSpine A3 or A4 thoracolumbar fractures with neurological deficits who were treated with EMIS or OS between June 2019 and July 2021 were extracted from the electronic database. Various clinical outcomes were compared between the 2 cohorts.</p><p><strong>Results: </strong>Among the 231 patients who were followed up for more than 2 years, 107 were in the EMIS cohort and 124 were in the OS cohort. Compared with the OS cohort, the EMIS cohort had longer operative time (p<0.05), but the intraoperative blood loss, incision length and hospital stay were significantly reduced (p<0.05). At both postoperative and final follow-up assessments, the EMIS cohort demonstrated significantly better visual analogue scale and Oswestry Disability Index outcomes compared to the OS cohort (p<0.05). Both cohorts maintained similar correction of spinal canal erosion rate, percentage of anterior vertebral height and sagittal Cobb angle after surgery and at the last follow-up (p>0.05). According to American Spinal Injury Association classification, the 2 cohorts had similar neurological recovery at the last follow-up (p>0.05).</p><p><strong>Conclusion: </strong>In comparison to OS, EMIS treatment for AOSpine A3 or A4 thoracolumbar fractures with neurological deficits has shown comparable clinical efficacy while significantly reducing surgical trauma.</p>","PeriodicalId":19269,"journal":{"name":"Neurospine","volume":" ","pages":"571-582"},"PeriodicalIF":3.6000,"publicationDate":"2025-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12242755/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Neurospine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.14245/ns.2449212.606","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/4/30 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: This study aimed to compare the clinical outcomes of patients with AOSpine A3 or A4 thoracolumbar fractures presenting with neurological deficits treated with endoscopic decompression combined with percutaneous pedicle screws fixation (endoscopic minimally invasive surgery, EMIS) or conventional open surgery (OS).
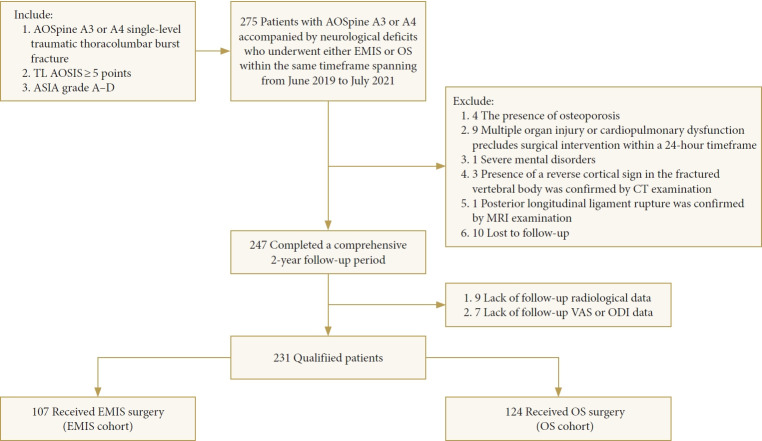
Methods: Data of patients with AOSpine A3 or A4 thoracolumbar fractures with neurological deficits who were treated with EMIS or OS between June 2019 and July 2021 were extracted from the electronic database. Various clinical outcomes were compared between the 2 cohorts.
Results: Among the 231 patients who were followed up for more than 2 years, 107 were in the EMIS cohort and 124 were in the OS cohort. Compared with the OS cohort, the EMIS cohort had longer operative time (p<0.05), but the intraoperative blood loss, incision length and hospital stay were significantly reduced (p<0.05). At both postoperative and final follow-up assessments, the EMIS cohort demonstrated significantly better visual analogue scale and Oswestry Disability Index outcomes compared to the OS cohort (p<0.05). Both cohorts maintained similar correction of spinal canal erosion rate, percentage of anterior vertebral height and sagittal Cobb angle after surgery and at the last follow-up (p>0.05). According to American Spinal Injury Association classification, the 2 cohorts had similar neurological recovery at the last follow-up (p>0.05).
Conclusion: In comparison to OS, EMIS treatment for AOSpine A3 or A4 thoracolumbar fractures with neurological deficits has shown comparable clinical efficacy while significantly reducing surgical trauma.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


