Development and Validation of a Nomogram for Predicting Adjacent Vertebral Fracture After Osteoporotic Vertebral Compression Fracture Surgery: A Multicenter Retrospective Cohort Study.
{"title":"Development and Validation of a Nomogram for Predicting Adjacent Vertebral Fracture After Osteoporotic Vertebral Compression Fracture Surgery: A Multicenter Retrospective Cohort Study.","authors":"Hanwen Cheng, Huilong Wen, Yong Ma, Zhuojie Liu, Haoyu Wu, Lajing Luowu, Yong Xiao, Lianbin Liang, Fanjie Kong, Longyi Xiao, Chunhai Li","doi":"10.14245/ns.2449338.669","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>Osteoporotic vertebral compression fractures (OVCFs) are a major public health concern. While percutaneous vertebral augmentation (PVA) is an effective treatment for OVCF, adjacent vertebral fractures (AVF) often occur post-PVA, adversely affecting treatment outcomes. This study aims to develop a nomogram for predicting AVF risk using multicenter data to aid clinical decision-making for OVCF patients.</p><p><strong>Methods: </strong>We retrospectively analyzed patients who underwent PVA at 3 hospitals between 2017 and 2022. The cohort was divided into a training set (80%) and a validation set (20%). Independent risk factors for AVF were identified using LASSO (least absolute shrinkage and selection operator) and logistic regression. Seven significant factors were: bone mineral density, diabetes, total fractured vertebrae, intravertebral vacuum cleft sign, recovery of local kyphosis angle, regular aerobic exercise, and lumbar brace use.</p><p><strong>Results: </strong>Among the 483 patients, 52 (10.76%) developed adjacent vertebral refractures within 2 years. The nomogram demonstrated high predictive accuracy, with area under the curves of 89.21% in the training set and 98.33% in the validation set.</p><p><strong>Conclusion: </strong>This pioneering nomogram, incorporating baseline, surgical, and postoperative factors, provides valuable guidance for spine surgeons in preoperative planning and postoperative management, enabling personalized prognosis and rehabilitation for OVCF patients.</p>","PeriodicalId":19269,"journal":{"name":"Neurospine","volume":" ","pages":"592-602"},"PeriodicalIF":3.6000,"publicationDate":"2025-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12242734/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Neurospine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.14245/ns.2449338.669","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/4/16 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: Osteoporotic vertebral compression fractures (OVCFs) are a major public health concern. While percutaneous vertebral augmentation (PVA) is an effective treatment for OVCF, adjacent vertebral fractures (AVF) often occur post-PVA, adversely affecting treatment outcomes. This study aims to develop a nomogram for predicting AVF risk using multicenter data to aid clinical decision-making for OVCF patients.
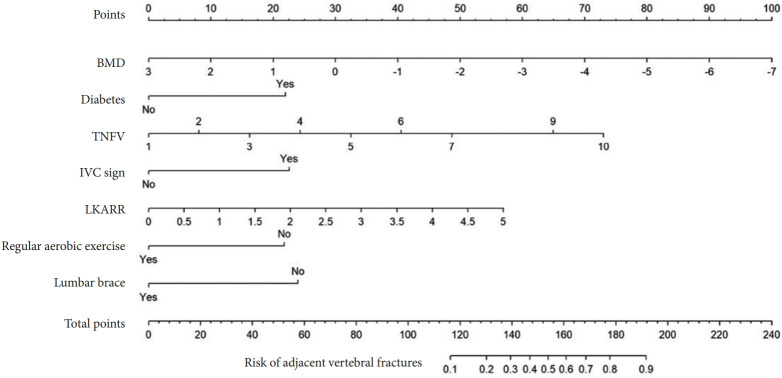
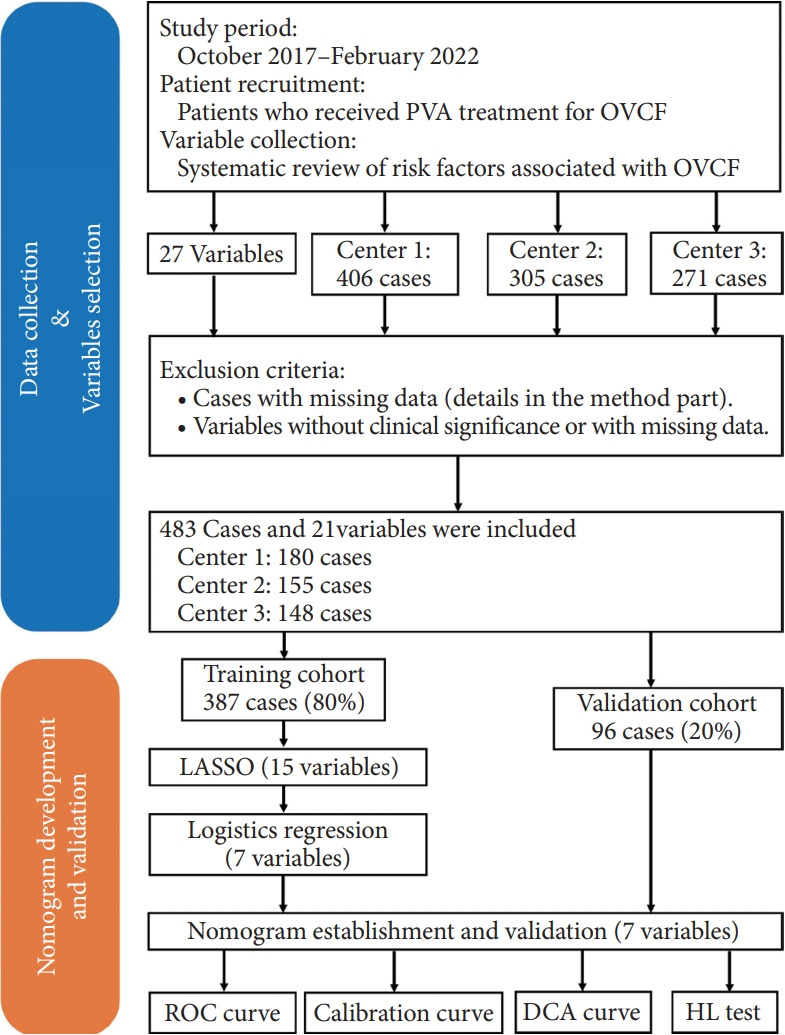
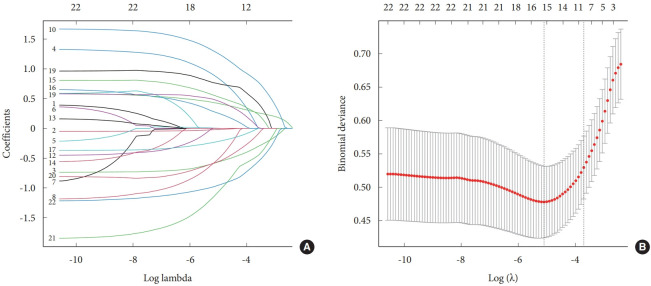
Methods: We retrospectively analyzed patients who underwent PVA at 3 hospitals between 2017 and 2022. The cohort was divided into a training set (80%) and a validation set (20%). Independent risk factors for AVF were identified using LASSO (least absolute shrinkage and selection operator) and logistic regression. Seven significant factors were: bone mineral density, diabetes, total fractured vertebrae, intravertebral vacuum cleft sign, recovery of local kyphosis angle, regular aerobic exercise, and lumbar brace use.
Results: Among the 483 patients, 52 (10.76%) developed adjacent vertebral refractures within 2 years. The nomogram demonstrated high predictive accuracy, with area under the curves of 89.21% in the training set and 98.33% in the validation set.
Conclusion: This pioneering nomogram, incorporating baseline, surgical, and postoperative factors, provides valuable guidance for spine surgeons in preoperative planning and postoperative management, enabling personalized prognosis and rehabilitation for OVCF patients.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


