{"title":"Early detection of cardiac impairment and prediction of right ventricular hypertrophy in patients with connective tissue disease.","authors":"Jiayan Shen, Guangrong Xiao, Shuqing Fang, Haohao Yang, Zheren Zhao, Yun Xu, Meng Jiang, Song Zhong","doi":"10.3892/br.2025.1970","DOIUrl":null,"url":null,"abstract":"<p><p>Progressive right ventricle (RV) failure and death in connective tissue disease (CTD) are related to RV hypertrophy (RVH) and dilation, irrespective of pulmonary arterial hypertension (PAH). Therefore, detecting cardiac impairment before RVH and determining RVH predictors is crucial for timely intervention. The present prospective cohort study aimed to identify cardiac markers that occur before RVH and to investigate predictors of RVH. CTD was diagnosed based on clinical features, laboratory findings and imaging data. The cardiac functions of patients with CTD were evaluated using echocardiography, cardiovascular magnetic resonance (CMR) and multi-modality cardiac imaging studies, including RV wall thickness, systolic functions, late gadolinium enhancement, T1 maps and biventricular strain analysis. A total of 52 patients with CTD with non-right ventricular hypertrophy (non-RVH), 34 patients with RVH and 50 healthy individuals were prospectively included. The impaired cardiac indices in patients with RVH included RV ejection fraction, ventricular dimensions, global myocardial deformation, late gadolinium enhancement and ventricular extracellular volume (ECV). The cardiac death rate did not differ significantly between the RVH and non-RVH groups (P=0.14). Conventional parameters, including serum cardiac markers and the left ventricular ejection fraction, showed no significant changes in the non-RVH group compared with the control group. Regarding fibrosis assessment using CMR, an elevated native T1 value (1,362±72 msec in the non-RVH group vs. 1,268±42 in the control group; P<0.001) and ECV (31±4% in the non-RVH group vs. 25±3% in the control group; P<0.001) were observed. By contrast, T1 myocardium/msec 15 min post-contrast of the left ventricle in the RVH group was significantly decreased compared with that in the non-RVH group, indicating an increase in the extracellular matrix at this stage. RVH was predicted by pulmonary arterial pressure (PAP) in patients in the non-RVH group (t-statistic, 2.84; P=0.01), whereas after RVH presentation, RV end-systolic volume (RVESV) became a progression predictor of RVH (t-statistic, 7.98; P<0.0001). No other cardiac imaging or laboratory findings predicted RVH. To the best of our knowledge, the present study was the first to highlight the non-invasive detection of cardiac tissue impairment using CMR and provide support for cardiac treatment initiation before RVH detection. The predictors of RVH vary with the heart disease stage. PAP in the non-RVH stage and incompetence of RVESV in the RVH stage predicted the progression of RVH. The present study was part of a clinical trial (NCT03271385), which was registered on July 1, 2017, and started on September 1, 2017.</p>","PeriodicalId":8863,"journal":{"name":"Biomedical reports","volume":"22 5","pages":"92"},"PeriodicalIF":1.9000,"publicationDate":"2025-03-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11995382/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Biomedical reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3892/br.2025.1970","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/5/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"MEDICINE, RESEARCH & EXPERIMENTAL","Score":null,"Total":0}
引用次数: 0
Abstract
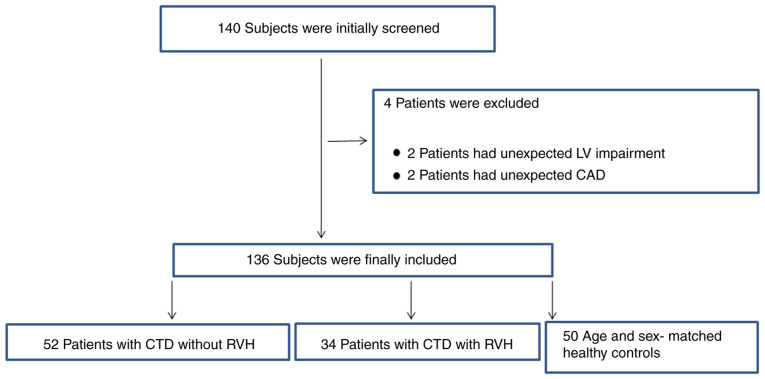
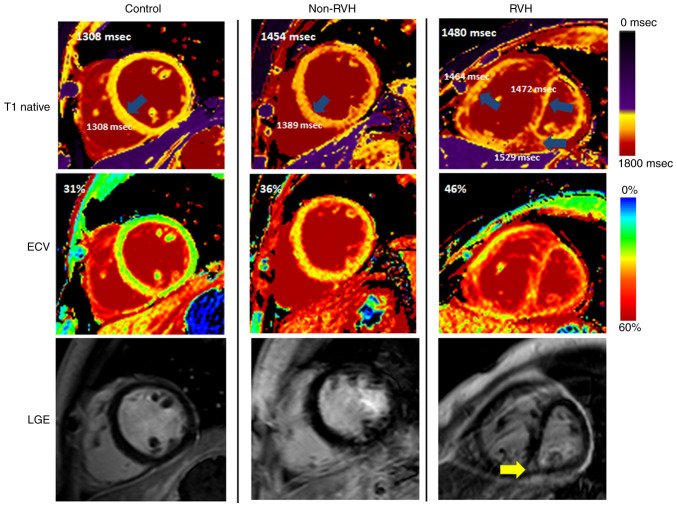
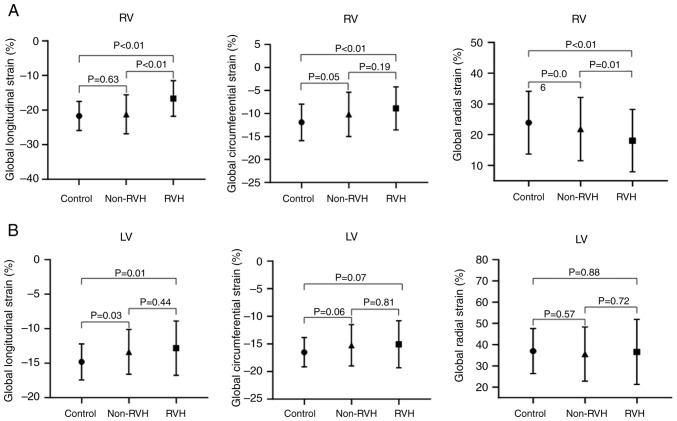
Progressive right ventricle (RV) failure and death in connective tissue disease (CTD) are related to RV hypertrophy (RVH) and dilation, irrespective of pulmonary arterial hypertension (PAH). Therefore, detecting cardiac impairment before RVH and determining RVH predictors is crucial for timely intervention. The present prospective cohort study aimed to identify cardiac markers that occur before RVH and to investigate predictors of RVH. CTD was diagnosed based on clinical features, laboratory findings and imaging data. The cardiac functions of patients with CTD were evaluated using echocardiography, cardiovascular magnetic resonance (CMR) and multi-modality cardiac imaging studies, including RV wall thickness, systolic functions, late gadolinium enhancement, T1 maps and biventricular strain analysis. A total of 52 patients with CTD with non-right ventricular hypertrophy (non-RVH), 34 patients with RVH and 50 healthy individuals were prospectively included. The impaired cardiac indices in patients with RVH included RV ejection fraction, ventricular dimensions, global myocardial deformation, late gadolinium enhancement and ventricular extracellular volume (ECV). The cardiac death rate did not differ significantly between the RVH and non-RVH groups (P=0.14). Conventional parameters, including serum cardiac markers and the left ventricular ejection fraction, showed no significant changes in the non-RVH group compared with the control group. Regarding fibrosis assessment using CMR, an elevated native T1 value (1,362±72 msec in the non-RVH group vs. 1,268±42 in the control group; P<0.001) and ECV (31±4% in the non-RVH group vs. 25±3% in the control group; P<0.001) were observed. By contrast, T1 myocardium/msec 15 min post-contrast of the left ventricle in the RVH group was significantly decreased compared with that in the non-RVH group, indicating an increase in the extracellular matrix at this stage. RVH was predicted by pulmonary arterial pressure (PAP) in patients in the non-RVH group (t-statistic, 2.84; P=0.01), whereas after RVH presentation, RV end-systolic volume (RVESV) became a progression predictor of RVH (t-statistic, 7.98; P<0.0001). No other cardiac imaging or laboratory findings predicted RVH. To the best of our knowledge, the present study was the first to highlight the non-invasive detection of cardiac tissue impairment using CMR and provide support for cardiac treatment initiation before RVH detection. The predictors of RVH vary with the heart disease stage. PAP in the non-RVH stage and incompetence of RVESV in the RVH stage predicted the progression of RVH. The present study was part of a clinical trial (NCT03271385), which was registered on July 1, 2017, and started on September 1, 2017.
期刊介绍:
Biomedical Reports is a monthly, peer-reviewed journal, dedicated to publishing research across all fields of biology and medicine, including pharmacology, pathology, gene therapy, genetics, microbiology, neurosciences, infectious diseases, molecular cardiology and molecular surgery. The journal provides a home for original research, case reports and review articles.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


