Relationship between Preoperative Adjacent Disc Height and the Occurrence of Adjacent Vertebral Body Fractures after Balloon Kyphoplasty for Osteoporotic Fractures at the Thoracolumbar Junction.
{"title":"Relationship between Preoperative Adjacent Disc Height and the Occurrence of Adjacent Vertebral Body Fractures after Balloon Kyphoplasty for Osteoporotic Fractures at the Thoracolumbar Junction.","authors":"Motonori Ishii, Yusuke Nishimura, Yu Yamamoto, Yoshitaka Nagashima, Takafumi Tanei, Masahito Hara, Masakazu Takayasu, Ryuta Saito","doi":"10.2176/jns-nmc.2024-0200","DOIUrl":null,"url":null,"abstract":"<p><p>Adjacent vertebral fractures after balloon kyphoplasty are speculated to occur in association with increased mechanical pressure due to rigid cement-augmented vertebrae. This study aimed to clarify whether adjacent vertebral fractures are more likely to occur after balloon kyphoplasty for osteoporotic vertebral fractures when the intervening adjacent disc degeneration is advanced. We retrospectively reviewed the findings for 99 patients who underwent balloon kyphoplasty for the first-ever osteoporotic vertebral fracture at the thoracolumbar junction levels (T11-L2). Radiological parameters and clinical data were compared for the cranial and caudal vertebrae between the groups with and without adjacent vertebral fractures within 1 year postoperatively. Postoperative adjacent vertebral fractures occurred in 20 patients (12 cranial adjacent vertebral fractures and eight caudal adjacent vertebral fractures). The cranial mean disc height was 5.87 ± 1.48 mm in the cranial adjacent vertebral fracture group and 7.98 ± 1.73 mm in the non-cranial adjacent vertebral fracture group (p < 0.01), and the caudal mean disc height was 6.24 ± 1.83 mm in the caudal adjacent vertebral fracture group and 9.55 ± 2.03 mm in the non-caudal adjacent vertebral fracture group (p < 0.01). According to receiver operating characteristic analysis, the optimized cutoff values of cranial mean disc height for cranial adjacent vertebral fracture occurrence and caudal mean disc height for caudal adjacent vertebral fracture occurrence were 6.37 mm and 7.70 mm, respectively. Multiple logistic regression models showed increased odds ratios for low disc height and large cement volume for cranial adjacent vertebral fractures and low disc height and cement leakage for caudal adjacent vertebral fractures. In conclusion, patients with advanced preoperative degeneration of the adjacent disc showed a higher incidence of adjacent vertebral fracture after balloon kyphoplasty.</p>","PeriodicalId":19225,"journal":{"name":"Neurologia medico-chirurgica","volume":" ","pages":"113-119"},"PeriodicalIF":2.3000,"publicationDate":"2025-03-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11968194/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Neurologia medico-chirurgica","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.2176/jns-nmc.2024-0200","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/2/10 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
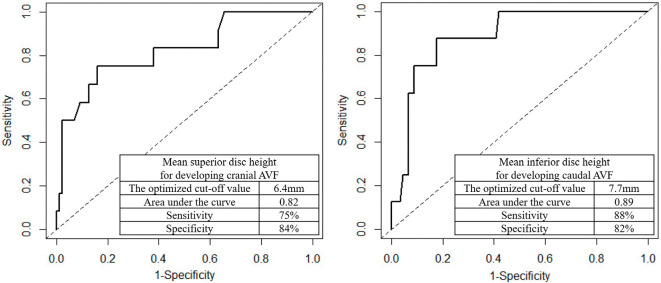
Adjacent vertebral fractures after balloon kyphoplasty are speculated to occur in association with increased mechanical pressure due to rigid cement-augmented vertebrae. This study aimed to clarify whether adjacent vertebral fractures are more likely to occur after balloon kyphoplasty for osteoporotic vertebral fractures when the intervening adjacent disc degeneration is advanced. We retrospectively reviewed the findings for 99 patients who underwent balloon kyphoplasty for the first-ever osteoporotic vertebral fracture at the thoracolumbar junction levels (T11-L2). Radiological parameters and clinical data were compared for the cranial and caudal vertebrae between the groups with and without adjacent vertebral fractures within 1 year postoperatively. Postoperative adjacent vertebral fractures occurred in 20 patients (12 cranial adjacent vertebral fractures and eight caudal adjacent vertebral fractures). The cranial mean disc height was 5.87 ± 1.48 mm in the cranial adjacent vertebral fracture group and 7.98 ± 1.73 mm in the non-cranial adjacent vertebral fracture group (p < 0.01), and the caudal mean disc height was 6.24 ± 1.83 mm in the caudal adjacent vertebral fracture group and 9.55 ± 2.03 mm in the non-caudal adjacent vertebral fracture group (p < 0.01). According to receiver operating characteristic analysis, the optimized cutoff values of cranial mean disc height for cranial adjacent vertebral fracture occurrence and caudal mean disc height for caudal adjacent vertebral fracture occurrence were 6.37 mm and 7.70 mm, respectively. Multiple logistic regression models showed increased odds ratios for low disc height and large cement volume for cranial adjacent vertebral fractures and low disc height and cement leakage for caudal adjacent vertebral fractures. In conclusion, patients with advanced preoperative degeneration of the adjacent disc showed a higher incidence of adjacent vertebral fracture after balloon kyphoplasty.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


