George Athanasios Karpouzas, Bianca Papotti, Sarah R Ormseth, Marcella Palumbo, Elizabeth Hernandez, Maria Pia Adorni, Francesca Zimetti, Nicoletta Ronda
{"title":"Changes in serum cholesterol loading capacity are linked to coronary atherosclerosis progression in rheumatoid arthritis.","authors":"George Athanasios Karpouzas, Bianca Papotti, Sarah R Ormseth, Marcella Palumbo, Elizabeth Hernandez, Maria Pia Adorni, Francesca Zimetti, Nicoletta Ronda","doi":"10.1136/rmdopen-2024-004991","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>Excess cholesterol loading on arterial macrophages is linked to foam cell formation, atherosclerosis and cardiovascular risk in rheumatoid arthritis (RA). However, the effect of changes in cholesterol loading on coronary plaque trajectory and the impact of RA therapies on this relationship are unknown. We investigated the association between variations in cholesterol loading capacity (CLC) over time and atherosclerosis progression.</p><p><strong>Methods: </strong>In a prospective observational cohort study, coronary CT angiography evaluated atherosclerosis (non-calcified, partially calcified or fully calcified plaques and coronary artery calcium (CAC) score) in 100 patients with RA without cardiovascular disease at baseline and 6.9±0.4 years later. The presence of ≥5 plaques and lesions rendering >50% stenosis was considered an extensive and obstructive disease, respectively. Serum CLC was measured on human THP-1 monocyte-derived macrophages with a fluorometric assay.</p><p><strong>Results: </strong>Mean CLC change (follow-up CLC-baseline CLC) was 1.54 (SD 3.69) μg cholesterol/mg protein. In models adjusting for atherosclerotic cardiovascular disease risk score, baseline plaque and other relevant covariates, CLC change (per SD unit increase) is associated with a higher likelihood of progression of non-calcified (OR 2.55, 95% CI 1.22 to 5.35), fully calcified plaque (OR 3.10, 95% CI 1.67 to 5.76), CAC (OR 1.80, 95% CI 1.18 to 2.74) and new extensive or obstructive disease (OR 2.43, 95% CI 1.11 to 5.34). Exposure to prednisone unfavourably influenced, while biologics and statins favourably affected the relationship between CLC change and atherosclerosis progression (all p-for-interactions ≤0.048).</p><p><strong>Conclusion: </strong>CLC change is associated with atherosclerosis progression in a dose-dependent manner, including lipid-rich non-calcified plaques and extensive or obstructive disease that yield the greatest cardiovascular risk.</p>","PeriodicalId":21396,"journal":{"name":"RMD Open","volume":"10 4","pages":""},"PeriodicalIF":4.7000,"publicationDate":"2024-12-24","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11683967/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"RMD Open","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1136/rmdopen-2024-004991","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"RHEUMATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: Excess cholesterol loading on arterial macrophages is linked to foam cell formation, atherosclerosis and cardiovascular risk in rheumatoid arthritis (RA). However, the effect of changes in cholesterol loading on coronary plaque trajectory and the impact of RA therapies on this relationship are unknown. We investigated the association between variations in cholesterol loading capacity (CLC) over time and atherosclerosis progression.
Methods: In a prospective observational cohort study, coronary CT angiography evaluated atherosclerosis (non-calcified, partially calcified or fully calcified plaques and coronary artery calcium (CAC) score) in 100 patients with RA without cardiovascular disease at baseline and 6.9±0.4 years later. The presence of ≥5 plaques and lesions rendering >50% stenosis was considered an extensive and obstructive disease, respectively. Serum CLC was measured on human THP-1 monocyte-derived macrophages with a fluorometric assay.
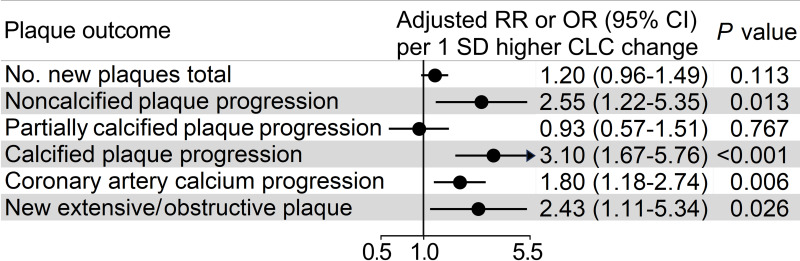
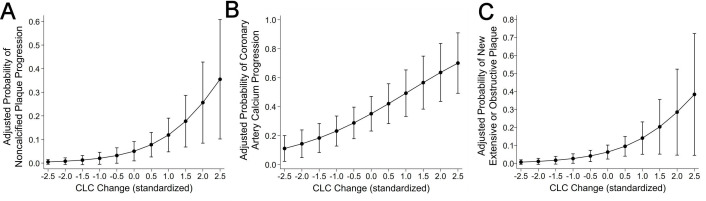
Results: Mean CLC change (follow-up CLC-baseline CLC) was 1.54 (SD 3.69) μg cholesterol/mg protein. In models adjusting for atherosclerotic cardiovascular disease risk score, baseline plaque and other relevant covariates, CLC change (per SD unit increase) is associated with a higher likelihood of progression of non-calcified (OR 2.55, 95% CI 1.22 to 5.35), fully calcified plaque (OR 3.10, 95% CI 1.67 to 5.76), CAC (OR 1.80, 95% CI 1.18 to 2.74) and new extensive or obstructive disease (OR 2.43, 95% CI 1.11 to 5.34). Exposure to prednisone unfavourably influenced, while biologics and statins favourably affected the relationship between CLC change and atherosclerosis progression (all p-for-interactions ≤0.048).
Conclusion: CLC change is associated with atherosclerosis progression in a dose-dependent manner, including lipid-rich non-calcified plaques and extensive or obstructive disease that yield the greatest cardiovascular risk.
期刊介绍:
RMD Open publishes high quality peer-reviewed original research covering the full spectrum of musculoskeletal disorders, rheumatism and connective tissue diseases, including osteoporosis, spine and rehabilitation. Clinical and epidemiological research, basic and translational medicine, interesting clinical cases, and smaller studies that add to the literature are all considered.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


