{"title":"Comparing the Circumplex Model and the Paradigmatic Framework","authors":"Armeda Stevenson Wojciak, David H. Olson","doi":"10.1111/jftr.12604","DOIUrl":null,"url":null,"abstract":"<p>The circumplex model of marital and family systems (Olson et al., <span>1979</span>) was developed to bridge the gap between theory, research, and clinical practice (Olson et al., <span>1989</span>). The Circumplex Model (CM) is based on theoretical ideas from a variety of theorists and researchers who have worked independently (see Olson et al., <span>2019</span> for a comprehensive list). From this work, a conceptual clustering of over 200 concepts from both the general and family systems fields yielded three dimensions (cohesion, flexibility, and communication) that comprise the dimensions of the Circumplex Model (Olson et al., <span>1979</span>).</p><p>The Circumplex Model is a theoretical model, but there is also a self-report assessment called the Family Adaptability and Cohesion Evaluation Scales (FACES I, II, IIII, IV) and an observational rating scale called the Clinical Rating Scale (CRS) that was created to measure the three dimensions. These measures have been used in empirical studies, clinical assessment, and treatment planning. FACES and the CRS have also been used to evaluate outcomes of couple and family therapy (Olson, <span>2000</span>). To date, there have been over 1200 published studies that have used the Circumplex Model as the theoretical foundation (Olson et al., <span>2019</span>). Global interest in using FACES has steadily increased (Olson et al., <span>2019</span>), indicating the universal applicability of the model in diverse couple and family contexts.</p><p>The prolific and ongoing translation of the Circumplex Model and accompanying measures is based in part on the direct applicability of the three hypotheses driving the Circumplex Model. The central hypothesis is: <i>balanced couples and families function more adequately than unbalanced couples and families</i>. The second hypothesis is: <i>balanced couples and families have more positive communication skills than unbalanced couples and families</i>. The third hypotheses is: <i>there will be changes in levels of cohesion and flexibility to deal with stress</i>. This last hypothesis ensures that the Circumplex Model is a dynamic model that can be useful to understand couples and families as they encounter different life experiences and developmental trajectories. Changes can be tracked across the five-by-five map (Olson et al., <span>2019</span>), which creates 25 systemic types. As illustrated in the Circumplex Model (see Figure 1), there are nine Balanced types, four Unbalanced types, and 12 Mid Range types.</p><p>Furthermore, FACES IV also provides a <i>communication scale</i> to better understand the way communication facilitates or inhibits family functioning. FACES IV also includes a <i>couple/family satisfaction scale</i> to examine an outcome measure that is specific to the couple or family completing the measure. Cumulatively, the Circumplex Model has bridged the theory, research, and clinical practice gap and continues to evolve and show applicability across diverse family contexts.</p><p>To illustrate the clinical application of FACES IV and the CRS, we will provide a brief case example, as well as a baseline assessment and 6 months into treatment assessment of FACES IV, to demonstrate FACES ability to track change over time (see Figure 2).</p><p>The last 3 years for the Jones family have resulted in a few significant transitions. The couple has three children: Jesse (14 years old), Sam (10 years old), and Jordan (8 years old). Two and a half years ago, the parents decided to separate to see if they could work on their relationship and if the mom could get support and address her drinking problem. Unfortunately, despite concerted efforts, the couple decided to divorce.</p><p>After the divorce, the dad has primary custody of the three children. The dad was and continues to be the primary provider for the family. The mom was a full-time parent prior to the divorce, and as her alcohol addiction progressed after the separation and divorce, she has less and less contact with the children. Consequently, the separation and divorce, and transition to more time with their dad and less time with their mom, has been difficult.</p><p>Jesse, a teenager, has been shifting away from her family whenever she can, especially at the dismay of her two younger siblings. The two youngest siblings openly talk about missing their mom and wish that their dad was not so stressed all the time. They also wish that their older sister would spend more time with them like she use to do. The dad wants to do what is best for his kids but is not sure what that looks like. He feels like he is floundering. Six months ago, he decided to bring his kids in for family therapy.</p><p>The therapist administered FACES IV to the dad and daughters, and completed the Clinical Rating Scale. The therapist first identified that the mom was currently <i>disengaged</i> due to her alcohol problem and inconsistent communication and connection with her kids. Jesse also appeared <i>disengaged</i>. The therapist speculated that this may be explained by both adolescent development and the family transitions that can be addressed throughout the course of family therapy.</p><p>At the time of assessment, FACES IV indicated that the family was <i>somewhat connected</i> and <i>very flexible</i>. The Clinical Rating Scale helped to show that the family as a unit had more separate time than together time, with the exception of the two younger. They spent a lot of time together and more time with their dad than did the oldest girl. As a result of this greater level of closeness, the younger kids had greater loyalty to their dad, but they reported feeling torn in their loyalty because they miss their mom and want her around more.</p><p>The dad has tried to navigate his new sole leadership and discipline role in the family in a way that engages with his kids, specifically trying to engage Jesse the most. When she does not engage with him, he consequently is firmer with the younger kids. The younger kids felt that their father tried to engage them in important family discussions like household chores and access to technology, but feel like Jesse gets all the attention and effort. The therapist observes that the dad is fairly consistent in his role and his rules are pretty clear, but he can use support to be more consistent across all kids.</p><p>After 6 months of family therapy, in which the therapist and family worked on creating a safe environment for the dad and kids to process the changes in their family together and work together to identify new roles, rules, and ways of interaction, the family communication improved, particularly between the dad and Jesse. Consequently, the family has seen a shift in their level of cohesion, to that of <i>connected</i> across the dad and kids and a slight shift in flexibility by all family members (see Figure 2), but still rated as <i>very flexible</i>. This shift did not change too much because the father was already trying to be flexible with the family as he knew his kids were going through a lot. Instead, the therapist worked with him to be more intentional in discerning what aspects of parenting he wanted/needed to be flexible in for his family. This case example illustrates the way in which the Circumplex Model can provide a snapshot in time to understand the family and what needs to be addressed to support the family and to see objective improvement.</p><p>The Paradigmatic Framework was created with concepts and principles from general system theory to help understand human systems (Constantine, <span>2025</span>). A paradigm is both a model and a world view. Constantine has provided examples of how the Paradigmatic Framework was systematically developed and has provided multiple theoretical applications of the Paradigmatic Framework within family therapy (Constantine, <span>1984</span>; Constantine & Israel, <span>1985</span>) and adolescent development in families (Constantine, <span>1987</span>).</p><p>Both the Circumplex Model and the Paradigmatic Framework were created to understand couple and family relationships as complex and dynamic systems. We have described the strengths of both the Circumplex Model and the Paradigmatic Framework and have highlighted the ways in which the two models share some commonality and ways in which they are different. The CM was also created to bridge the gap between theory, research, and practice and this is a next step for the Paradigmatic Framework.</p>","PeriodicalId":47446,"journal":{"name":"Journal of Family Theory & Review","volume":"17 2","pages":"207-212"},"PeriodicalIF":4.5000,"publicationDate":"2024-12-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/jftr.12604","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Family Theory & Review","FirstCategoryId":"90","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/jftr.12604","RegionNum":1,"RegionCategory":"社会学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"FAMILY STUDIES","Score":null,"Total":0}
引用次数: 0
Abstract
The circumplex model of marital and family systems (Olson et al., 1979) was developed to bridge the gap between theory, research, and clinical practice (Olson et al., 1989). The Circumplex Model (CM) is based on theoretical ideas from a variety of theorists and researchers who have worked independently (see Olson et al., 2019 for a comprehensive list). From this work, a conceptual clustering of over 200 concepts from both the general and family systems fields yielded three dimensions (cohesion, flexibility, and communication) that comprise the dimensions of the Circumplex Model (Olson et al., 1979).
The Circumplex Model is a theoretical model, but there is also a self-report assessment called the Family Adaptability and Cohesion Evaluation Scales (FACES I, II, IIII, IV) and an observational rating scale called the Clinical Rating Scale (CRS) that was created to measure the three dimensions. These measures have been used in empirical studies, clinical assessment, and treatment planning. FACES and the CRS have also been used to evaluate outcomes of couple and family therapy (Olson, 2000). To date, there have been over 1200 published studies that have used the Circumplex Model as the theoretical foundation (Olson et al., 2019). Global interest in using FACES has steadily increased (Olson et al., 2019), indicating the universal applicability of the model in diverse couple and family contexts.
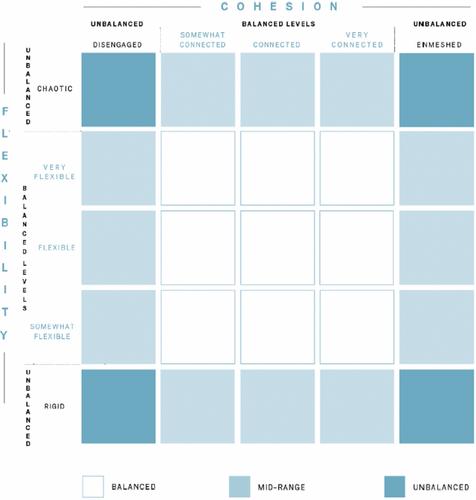
The prolific and ongoing translation of the Circumplex Model and accompanying measures is based in part on the direct applicability of the three hypotheses driving the Circumplex Model. The central hypothesis is: balanced couples and families function more adequately than unbalanced couples and families. The second hypothesis is: balanced couples and families have more positive communication skills than unbalanced couples and families. The third hypotheses is: there will be changes in levels of cohesion and flexibility to deal with stress. This last hypothesis ensures that the Circumplex Model is a dynamic model that can be useful to understand couples and families as they encounter different life experiences and developmental trajectories. Changes can be tracked across the five-by-five map (Olson et al., 2019), which creates 25 systemic types. As illustrated in the Circumplex Model (see Figure 1), there are nine Balanced types, four Unbalanced types, and 12 Mid Range types.
Furthermore, FACES IV also provides a communication scale to better understand the way communication facilitates or inhibits family functioning. FACES IV also includes a couple/family satisfaction scale to examine an outcome measure that is specific to the couple or family completing the measure. Cumulatively, the Circumplex Model has bridged the theory, research, and clinical practice gap and continues to evolve and show applicability across diverse family contexts.
To illustrate the clinical application of FACES IV and the CRS, we will provide a brief case example, as well as a baseline assessment and 6 months into treatment assessment of FACES IV, to demonstrate FACES ability to track change over time (see Figure 2).
The last 3 years for the Jones family have resulted in a few significant transitions. The couple has three children: Jesse (14 years old), Sam (10 years old), and Jordan (8 years old). Two and a half years ago, the parents decided to separate to see if they could work on their relationship and if the mom could get support and address her drinking problem. Unfortunately, despite concerted efforts, the couple decided to divorce.
After the divorce, the dad has primary custody of the three children. The dad was and continues to be the primary provider for the family. The mom was a full-time parent prior to the divorce, and as her alcohol addiction progressed after the separation and divorce, she has less and less contact with the children. Consequently, the separation and divorce, and transition to more time with their dad and less time with their mom, has been difficult.
Jesse, a teenager, has been shifting away from her family whenever she can, especially at the dismay of her two younger siblings. The two youngest siblings openly talk about missing their mom and wish that their dad was not so stressed all the time. They also wish that their older sister would spend more time with them like she use to do. The dad wants to do what is best for his kids but is not sure what that looks like. He feels like he is floundering. Six months ago, he decided to bring his kids in for family therapy.
The therapist administered FACES IV to the dad and daughters, and completed the Clinical Rating Scale. The therapist first identified that the mom was currently disengaged due to her alcohol problem and inconsistent communication and connection with her kids. Jesse also appeared disengaged. The therapist speculated that this may be explained by both adolescent development and the family transitions that can be addressed throughout the course of family therapy.
At the time of assessment, FACES IV indicated that the family was somewhat connected and very flexible. The Clinical Rating Scale helped to show that the family as a unit had more separate time than together time, with the exception of the two younger. They spent a lot of time together and more time with their dad than did the oldest girl. As a result of this greater level of closeness, the younger kids had greater loyalty to their dad, but they reported feeling torn in their loyalty because they miss their mom and want her around more.
The dad has tried to navigate his new sole leadership and discipline role in the family in a way that engages with his kids, specifically trying to engage Jesse the most. When she does not engage with him, he consequently is firmer with the younger kids. The younger kids felt that their father tried to engage them in important family discussions like household chores and access to technology, but feel like Jesse gets all the attention and effort. The therapist observes that the dad is fairly consistent in his role and his rules are pretty clear, but he can use support to be more consistent across all kids.
After 6 months of family therapy, in which the therapist and family worked on creating a safe environment for the dad and kids to process the changes in their family together and work together to identify new roles, rules, and ways of interaction, the family communication improved, particularly between the dad and Jesse. Consequently, the family has seen a shift in their level of cohesion, to that of connected across the dad and kids and a slight shift in flexibility by all family members (see Figure 2), but still rated as very flexible. This shift did not change too much because the father was already trying to be flexible with the family as he knew his kids were going through a lot. Instead, the therapist worked with him to be more intentional in discerning what aspects of parenting he wanted/needed to be flexible in for his family. This case example illustrates the way in which the Circumplex Model can provide a snapshot in time to understand the family and what needs to be addressed to support the family and to see objective improvement.
The Paradigmatic Framework was created with concepts and principles from general system theory to help understand human systems (Constantine, 2025). A paradigm is both a model and a world view. Constantine has provided examples of how the Paradigmatic Framework was systematically developed and has provided multiple theoretical applications of the Paradigmatic Framework within family therapy (Constantine, 1984; Constantine & Israel, 1985) and adolescent development in families (Constantine, 1987).
Both the Circumplex Model and the Paradigmatic Framework were created to understand couple and family relationships as complex and dynamic systems. We have described the strengths of both the Circumplex Model and the Paradigmatic Framework and have highlighted the ways in which the two models share some commonality and ways in which they are different. The CM was also created to bridge the gap between theory, research, and practice and this is a next step for the Paradigmatic Framework.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


