Kannan Sridharan, Muna Al Jufairi, Eman Al Ansari, Lulwa Alsadah, Howra Wasel
{"title":"Is fat-free mass-based gentamicin dosing regimen preferable than whole-body weight in neonates?","authors":"Kannan Sridharan, Muna Al Jufairi, Eman Al Ansari, Lulwa Alsadah, Howra Wasel","doi":"10.1002/ped4.12386","DOIUrl":null,"url":null,"abstract":"<p><strong>Importance: </strong>Body fluid dynamics and renal maturation status vary during the neonatal period. We hypothesized that differences in peak and trough gentamicin concentrations could be expected.</p><p><strong>Objective: </strong>To predict the peak and trough gentamicin concentrations in critically ill neonates and to predict the changes in the predicted peak plasma concentrations of gentamicin following fat-free mass dosing.</p><p><strong>Methods: </strong>Critically ill neonates that received gentamicin and have gentamicin concentration measured were recruited. Fat mass was estimated using skinfold thicknesses. Changes in the peak plasma concentrations (C<sub>max</sub>) using whole-body weight (estimated using the current dosing regimen) and predicted concentrations following the fat-free mass-based dosing were the outcome measures.</p><p><strong>Results: </strong>Eighty-nine critically ill neonates were recruited. Sub-therapeutic C<sub>max</sub> was estimated using the current dosing regimen in 32.6%, and 22.5% neonates following the first and second doses of gentamicin. Preterm neonates had significantly higher fat mass compared to term neonates. All except one had C<sub>max</sub> above 12 μg/ml after the first dose and all had after the second gentamicin dose following the predicted fat-free mass-based gentamicin dosing. The recommended doses are as follows: extreme preterm: 7.95 mg/kg every 48 h; very preterm: 7.30 mg/kg every 36-48 h; late preterm: 5.90 mg/kg every 36-48 h; and term neonates at 5.10 mg/kg every 24 h.</p><p><strong>Interpretation: </strong>Fat-free mass dosing may be considered for obtaining optimal therapeutic effects in the neonatal population.</p>","PeriodicalId":19992,"journal":{"name":"Pediatric Investigation","volume":"7 2","pages":"86-94"},"PeriodicalIF":2.0000,"publicationDate":"2023-06-08","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/f6/46/PED4-7-86.PMC10262884.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pediatric Investigation","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1002/ped4.12386","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/6/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"PEDIATRICS","Score":null,"Total":0}
引用次数: 0
Abstract
Importance: Body fluid dynamics and renal maturation status vary during the neonatal period. We hypothesized that differences in peak and trough gentamicin concentrations could be expected.
Objective: To predict the peak and trough gentamicin concentrations in critically ill neonates and to predict the changes in the predicted peak plasma concentrations of gentamicin following fat-free mass dosing.
Methods: Critically ill neonates that received gentamicin and have gentamicin concentration measured were recruited. Fat mass was estimated using skinfold thicknesses. Changes in the peak plasma concentrations (Cmax) using whole-body weight (estimated using the current dosing regimen) and predicted concentrations following the fat-free mass-based dosing were the outcome measures.
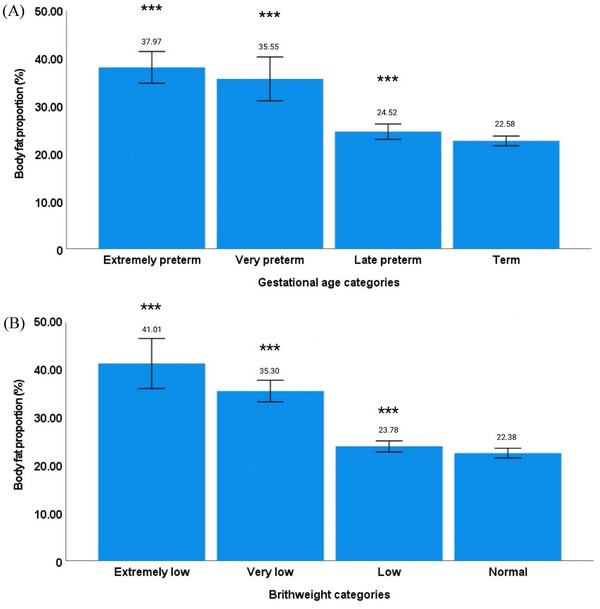
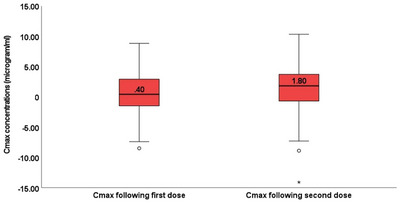
Results: Eighty-nine critically ill neonates were recruited. Sub-therapeutic Cmax was estimated using the current dosing regimen in 32.6%, and 22.5% neonates following the first and second doses of gentamicin. Preterm neonates had significantly higher fat mass compared to term neonates. All except one had Cmax above 12 μg/ml after the first dose and all had after the second gentamicin dose following the predicted fat-free mass-based gentamicin dosing. The recommended doses are as follows: extreme preterm: 7.95 mg/kg every 48 h; very preterm: 7.30 mg/kg every 36-48 h; late preterm: 5.90 mg/kg every 36-48 h; and term neonates at 5.10 mg/kg every 24 h.
Interpretation: Fat-free mass dosing may be considered for obtaining optimal therapeutic effects in the neonatal population.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


