{"title":"心力衰竭伴射血分数降低患者出院时的药物治疗模式和临床结果","authors":"Yuttana Wongsalap, Duangkamon Poolpun, Konrapee Keawhai, Napusson Kitpluem, Parichat Pansiri, Siriluck Malaimat, Vichai Senthong, Kirati Kengkla","doi":"10.1002/cdt3.59","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Background</h3>\n \n <p>This study aimed to assess the prescribing patterns of evidence-based pharmacotherapy and their association with clinical outcomes in patients with heart failure with reduced ejection fraction (HFrEF) in Thailand.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>A retrospective cohort study of patients with HFrEF was conducted. Treatment with a β-blocker and renin–angiotensin system inhibitors (RASIs) with or without mineralocorticoid receptor antagonists (MRAs) at discharge was regarded as guideline-directed medical therapy (GDMT). All others were considered non-GDMT. The primary endpoint was the composite of all-cause mortality or heart failure (HF) rehospitalization. Inverse-probability-treatment-weighted adjusted Cox proportional hazard models were used to examine the treatment effects.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>In total, 653 patients with HFrEF (mean age 64.1 ± 14.3 years; 55.9% male) were included. GDMT with β-blockers and RASIs with or without MRAs was prescribed at a rate of 35.4%. During a median of 1-year follow-up, 167 patients (27.5%) had a composite event, 81 patients (13.3%) had all-cause mortality, and 109 patients (18.0%) had HF rehospitalization. Patients treated with GDMT at discharge showed significantly lower rates of the primary endpoint (adjusted hazard ratio [HR] 0.63; 95% CI 0.44–0.89; <i>p</i> = 0.009) compared with patients who did not receive GDMT. The use of GDMT was also associated with a significantly lower risk of all-cause mortality (adjusted HR 0.59; 95% CI 0.36–0.98; <i>p</i> = 0.045) and HF rehospitalization (adjusted HR 0.65; 95% CI 0.43–0.96; <i>p</i> = 0.031).</p>\n </section>\n \n <section>\n \n <h3> Conclusions</h3>\n \n <p>For HFrEF treatment, GDMT initiation at hospital discharge was associated with a significantly reduced risk of all-cause mortality and HF rehospitalization. Nevertheless, prescribing GDMT remains underused, and it could be encouraged to improve HF outcomes in real-world settings.</p>\n </section>\n </div>","PeriodicalId":32096,"journal":{"name":"Chronic Diseases and Translational Medicine","volume":"9 2","pages":"154-163"},"PeriodicalIF":0.0000,"publicationDate":"2023-02-08","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/65/e9/CDT3-9-154.PMC10249177.pdf","citationCount":"0","resultStr":"{\"title\":\"Pharmacotherapy treatment patterns at hospital discharge and clinical outcomes among patients with heart failure with reduced ejection fraction\",\"authors\":\"Yuttana Wongsalap, Duangkamon Poolpun, Konrapee Keawhai, Napusson Kitpluem, Parichat Pansiri, Siriluck Malaimat, Vichai Senthong, Kirati Kengkla\",\"doi\":\"10.1002/cdt3.59\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n \\n \\n <section>\\n \\n <h3> Background</h3>\\n \\n <p>This study aimed to assess the prescribing patterns of evidence-based pharmacotherapy and their association with clinical outcomes in patients with heart failure with reduced ejection fraction (HFrEF) in Thailand.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Methods</h3>\\n \\n <p>A retrospective cohort study of patients with HFrEF was conducted. Treatment with a β-blocker and renin–angiotensin system inhibitors (RASIs) with or without mineralocorticoid receptor antagonists (MRAs) at discharge was regarded as guideline-directed medical therapy (GDMT). All others were considered non-GDMT. The primary endpoint was the composite of all-cause mortality or heart failure (HF) rehospitalization. Inverse-probability-treatment-weighted adjusted Cox proportional hazard models were used to examine the treatment effects.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Results</h3>\\n \\n <p>In total, 653 patients with HFrEF (mean age 64.1 ± 14.3 years; 55.9% male) were included. GDMT with β-blockers and RASIs with or without MRAs was prescribed at a rate of 35.4%. During a median of 1-year follow-up, 167 patients (27.5%) had a composite event, 81 patients (13.3%) had all-cause mortality, and 109 patients (18.0%) had HF rehospitalization. Patients treated with GDMT at discharge showed significantly lower rates of the primary endpoint (adjusted hazard ratio [HR] 0.63; 95% CI 0.44–0.89; <i>p</i> = 0.009) compared with patients who did not receive GDMT. The use of GDMT was also associated with a significantly lower risk of all-cause mortality (adjusted HR 0.59; 95% CI 0.36–0.98; <i>p</i> = 0.045) and HF rehospitalization (adjusted HR 0.65; 95% CI 0.43–0.96; <i>p</i> = 0.031).</p>\\n </section>\\n \\n <section>\\n \\n <h3> Conclusions</h3>\\n \\n <p>For HFrEF treatment, GDMT initiation at hospital discharge was associated with a significantly reduced risk of all-cause mortality and HF rehospitalization. Nevertheless, prescribing GDMT remains underused, and it could be encouraged to improve HF outcomes in real-world settings.</p>\\n </section>\\n </div>\",\"PeriodicalId\":32096,\"journal\":{\"name\":\"Chronic Diseases and Translational Medicine\",\"volume\":\"9 2\",\"pages\":\"154-163\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2023-02-08\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/65/e9/CDT3-9-154.PMC10249177.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Chronic Diseases and Translational Medicine\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/cdt3.59\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Chronic Diseases and Translational Medicine","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/cdt3.59","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
摘要
本研究旨在评估泰国心力衰竭伴射血分数降低(HFrEF)患者循证药物治疗的处方模式及其与临床结局的关系。方法对HFrEF患者进行回顾性队列研究。出院时使用β受体阻滞剂和肾素-血管紧张素系统抑制剂(RASIs)联合或不联合矿皮质激素受体拮抗剂(MRAs)进行治疗被视为指南导向药物治疗(GDMT)。所有其他的都被认为是非gdmt。主要终点是全因死亡率或心力衰竭(HF)再住院的综合。采用反概率处理加权校正Cox比例风险模型检验处理效果。结果共653例HFrEF患者(平均年龄64.1±14.3岁;55.9%为男性)。GDMT联合β受体阻滞剂和RASIs合并或不合并MRAs的处方率为35.4%。在中位1年的随访期间,167例患者(27.5%)出现复合事件,81例患者(13.3%)出现全因死亡,109例患者(18.0%)再次住院。出院时接受GDMT治疗的患者主要终点发生率显著降低(校正风险比[HR] 0.63;95% ci 0.44-0.89;p = 0.009),与未接受GDMT的患者相比。GDMT的使用还与全因死亡风险显著降低相关(调整后HR 0.59;95% ci 0.36-0.98;p = 0.045)和HF再住院(调整后HR 0.65;95% ci 0.43-0.96;p = 0.031)。结论:对于HF治疗,出院时开始GDMT与全因死亡率和HF再住院的风险显著降低相关。然而,处方GDMT仍未得到充分利用,可以鼓励在现实环境中改善心衰结果。
Pharmacotherapy treatment patterns at hospital discharge and clinical outcomes among patients with heart failure with reduced ejection fraction
Background
This study aimed to assess the prescribing patterns of evidence-based pharmacotherapy and their association with clinical outcomes in patients with heart failure with reduced ejection fraction (HFrEF) in Thailand.
Methods
A retrospective cohort study of patients with HFrEF was conducted. Treatment with a β-blocker and renin–angiotensin system inhibitors (RASIs) with or without mineralocorticoid receptor antagonists (MRAs) at discharge was regarded as guideline-directed medical therapy (GDMT). All others were considered non-GDMT. The primary endpoint was the composite of all-cause mortality or heart failure (HF) rehospitalization. Inverse-probability-treatment-weighted adjusted Cox proportional hazard models were used to examine the treatment effects.
Results
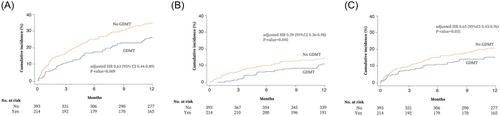
In total, 653 patients with HFrEF (mean age 64.1 ± 14.3 years; 55.9% male) were included. GDMT with β-blockers and RASIs with or without MRAs was prescribed at a rate of 35.4%. During a median of 1-year follow-up, 167 patients (27.5%) had a composite event, 81 patients (13.3%) had all-cause mortality, and 109 patients (18.0%) had HF rehospitalization. Patients treated with GDMT at discharge showed significantly lower rates of the primary endpoint (adjusted hazard ratio [HR] 0.63; 95% CI 0.44–0.89; p = 0.009) compared with patients who did not receive GDMT. The use of GDMT was also associated with a significantly lower risk of all-cause mortality (adjusted HR 0.59; 95% CI 0.36–0.98; p = 0.045) and HF rehospitalization (adjusted HR 0.65; 95% CI 0.43–0.96; p = 0.031).
Conclusions
For HFrEF treatment, GDMT initiation at hospital discharge was associated with a significantly reduced risk of all-cause mortality and HF rehospitalization. Nevertheless, prescribing GDMT remains underused, and it could be encouraged to improve HF outcomes in real-world settings.
期刊介绍:
This journal aims to promote progress from basic research to clinical practice and to provide a forum for communication among basic, translational, and clinical research practitioners and physicians from all relevant disciplines. Chronic diseases such as cardiovascular diseases, cancer, diabetes, stroke, chronic respiratory diseases (such as asthma and COPD), chronic kidney diseases, and related translational research. Topics of interest for Chronic Diseases and Translational Medicine include Research and commentary on models of chronic diseases with significant implications for disease diagnosis and treatment Investigative studies of human biology with an emphasis on disease Perspectives and reviews on research topics that discuss the implications of findings from the viewpoints of basic science and clinical practic.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


