Yanxin Liu , Jiang Wang , Tingting Liu , Kun Xiao , Peng Yan , Xiangqun Fang , Lixin Xie
{"title":"名为“ADPLCP”的诺模图预测模型用于预测老年人利奈唑胺相关血小板减少症","authors":"Yanxin Liu , Jiang Wang , Tingting Liu , Kun Xiao , Peng Yan , Xiangqun Fang , Lixin Xie","doi":"10.1016/j.jointm.2022.12.003","DOIUrl":null,"url":null,"abstract":"<div><h3>Background</h3><p>Linezolid-associated thrombocytopenia (LAT) leads to drug withdrawal associated with a poor prognosis. Some risk factors for LAT have been identified; however, the sample size of previous studies was small, data from elderly individuals are limited, and a simple risk score scale was not established to predict LAT at an early stage, making it difficult to identify and intervene in LAT at an early stage.</p></div><div><h3>Methods</h3><p>In this single-center retrospective case-control study, we enrolled elderly patients treated with linezolid in the intensive care unit from January 2015 to December 2020. All the data of enrolled patients, including demographic information and laboratory findings at baseline, were collected. We analyzed the incidence and risk factors for LAT and established a nomogram risk prediction model for LAT in the elderly population.</p></div><div><h3>Results</h3><p>A total of 428 elderly patients were enrolled, and the incidence of LAT was 35.5% (152/428). Age ≥80 years old (OR=1.980; 95% CI: 1.179–3.325; <em>P</em>=0.010), duration of linezolid ≥ 10 days (OR=1.100; 95% CI: 1.050–1.152; <em>P</em> <0.0001), platelet count at baseline (100–149×10<sup>9</sup>/L <em>vs</em>. ≥200×10<sup>9</sup>/L, OR=8.205, 95% CI: 4.419–15.232, <em>P</em> <0.0001; 150–199 ×10<sup>9</sup>/L <em>vs.</em> ≥200×10<sup>9</sup>/L, OR=3.067, 95% CI: 1.676–5.612, <em>P</em> <0.001), leukocyte count at baseline ≥16×10<sup>9</sup>/L (OR=2.580; 95% CI: 1.523–4.373; <em>P</em> <0.0001), creatinine clearance <50 mL/min (OR=2.323; 95% CI: 1.388–3.890; <em>P</em>=0.001), and total protein <60 g/L (OR=1.741; 95% CI: 1.039–2.919; <em>P</em>=0.035) were associated with LAT. The nomogram prediction model called “ADPLCP” (age, duration, platelet, leukocyte, creatinine clearance, protein) was established based on logistic regression. The area under the curve (AUC) of ADPLCP was 0.802 (95% CI: 0.748–0.856; <em>P</em> <0.0001), with 78.9% sensitivity and 69.2% specificity (cut-off was 108). Risk stratification for LAT was performed based on “ADPLCP.” Total points of <100 were defined as low risk, and the possibility of LAT was <32.0%. Total points of 100–150 were defined as medium risk, and the possibility of LAT was 32.0–67.5%. A total point >150 was defined as high risk, and the probability of LAT was >67.5%.</p></div><div><h3>Conclusions</h3><p>We created the ADPLCP risk score scale to predict the occurrence of LAT in elderly individuals. ADPLCP is simple and feasible and is helpful for the early determination of LAT to guide drug withdrawal or early intervention.</p></div>","PeriodicalId":73799,"journal":{"name":"Journal of intensive medicine","volume":"3 3","pages":"Pages 268-274"},"PeriodicalIF":0.0000,"publicationDate":"2023-07-31","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/04/0f/main.PMC10391562.pdf","citationCount":"0","resultStr":"{\"title\":\"Nomogram prediction model called “ADPLCP” for predicting linezolid-associated thrombocytopenia in elderly individuals\",\"authors\":\"Yanxin Liu , Jiang Wang , Tingting Liu , Kun Xiao , Peng Yan , Xiangqun Fang , Lixin Xie\",\"doi\":\"10.1016/j.jointm.2022.12.003\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div><h3>Background</h3><p>Linezolid-associated thrombocytopenia (LAT) leads to drug withdrawal associated with a poor prognosis. Some risk factors for LAT have been identified; however, the sample size of previous studies was small, data from elderly individuals are limited, and a simple risk score scale was not established to predict LAT at an early stage, making it difficult to identify and intervene in LAT at an early stage.</p></div><div><h3>Methods</h3><p>In this single-center retrospective case-control study, we enrolled elderly patients treated with linezolid in the intensive care unit from January 2015 to December 2020. All the data of enrolled patients, including demographic information and laboratory findings at baseline, were collected. We analyzed the incidence and risk factors for LAT and established a nomogram risk prediction model for LAT in the elderly population.</p></div><div><h3>Results</h3><p>A total of 428 elderly patients were enrolled, and the incidence of LAT was 35.5% (152/428). Age ≥80 years old (OR=1.980; 95% CI: 1.179–3.325; <em>P</em>=0.010), duration of linezolid ≥ 10 days (OR=1.100; 95% CI: 1.050–1.152; <em>P</em> <0.0001), platelet count at baseline (100–149×10<sup>9</sup>/L <em>vs</em>. ≥200×10<sup>9</sup>/L, OR=8.205, 95% CI: 4.419–15.232, <em>P</em> <0.0001; 150–199 ×10<sup>9</sup>/L <em>vs.</em> ≥200×10<sup>9</sup>/L, OR=3.067, 95% CI: 1.676–5.612, <em>P</em> <0.001), leukocyte count at baseline ≥16×10<sup>9</sup>/L (OR=2.580; 95% CI: 1.523–4.373; <em>P</em> <0.0001), creatinine clearance <50 mL/min (OR=2.323; 95% CI: 1.388–3.890; <em>P</em>=0.001), and total protein <60 g/L (OR=1.741; 95% CI: 1.039–2.919; <em>P</em>=0.035) were associated with LAT. The nomogram prediction model called “ADPLCP” (age, duration, platelet, leukocyte, creatinine clearance, protein) was established based on logistic regression. The area under the curve (AUC) of ADPLCP was 0.802 (95% CI: 0.748–0.856; <em>P</em> <0.0001), with 78.9% sensitivity and 69.2% specificity (cut-off was 108). Risk stratification for LAT was performed based on “ADPLCP.” Total points of <100 were defined as low risk, and the possibility of LAT was <32.0%. Total points of 100–150 were defined as medium risk, and the possibility of LAT was 32.0–67.5%. A total point >150 was defined as high risk, and the probability of LAT was >67.5%.</p></div><div><h3>Conclusions</h3><p>We created the ADPLCP risk score scale to predict the occurrence of LAT in elderly individuals. ADPLCP is simple and feasible and is helpful for the early determination of LAT to guide drug withdrawal or early intervention.</p></div>\",\"PeriodicalId\":73799,\"journal\":{\"name\":\"Journal of intensive medicine\",\"volume\":\"3 3\",\"pages\":\"Pages 268-274\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2023-07-31\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/04/0f/main.PMC10391562.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of intensive medicine\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://www.sciencedirect.com/science/article/pii/S2667100X2300004X\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of intensive medicine","FirstCategoryId":"1085","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S2667100X2300004X","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Nomogram prediction model called “ADPLCP” for predicting linezolid-associated thrombocytopenia in elderly individuals
Background
Linezolid-associated thrombocytopenia (LAT) leads to drug withdrawal associated with a poor prognosis. Some risk factors for LAT have been identified; however, the sample size of previous studies was small, data from elderly individuals are limited, and a simple risk score scale was not established to predict LAT at an early stage, making it difficult to identify and intervene in LAT at an early stage.
Methods
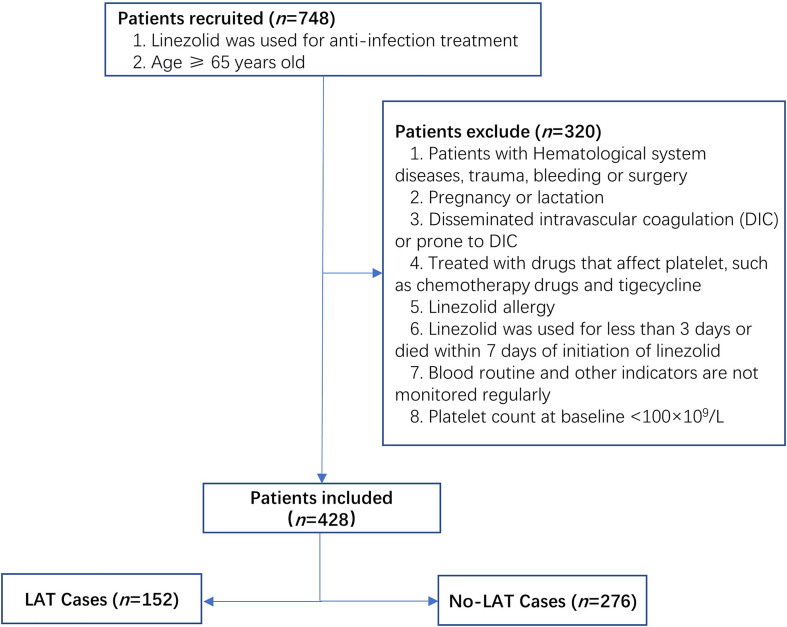
In this single-center retrospective case-control study, we enrolled elderly patients treated with linezolid in the intensive care unit from January 2015 to December 2020. All the data of enrolled patients, including demographic information and laboratory findings at baseline, were collected. We analyzed the incidence and risk factors for LAT and established a nomogram risk prediction model for LAT in the elderly population.
Results
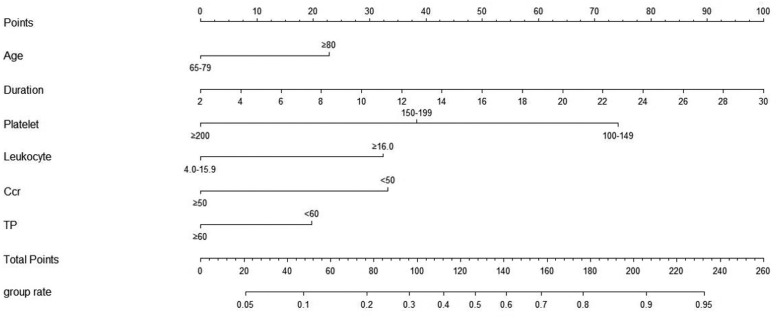
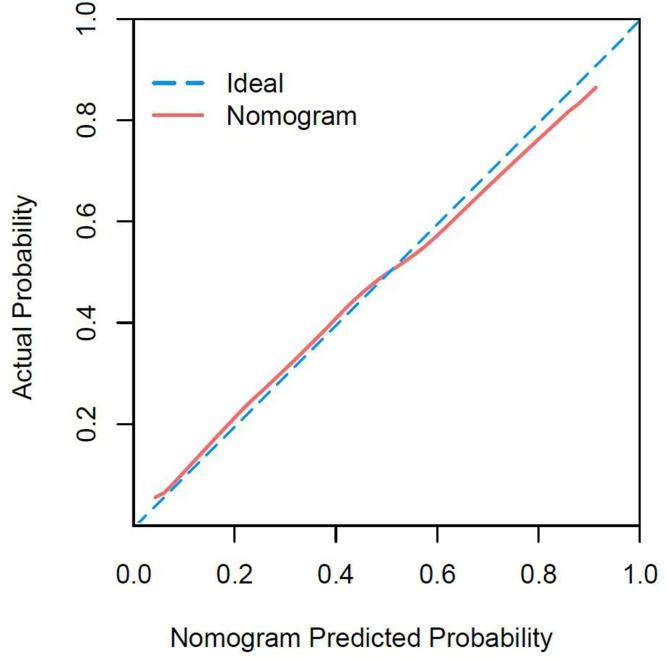
A total of 428 elderly patients were enrolled, and the incidence of LAT was 35.5% (152/428). Age ≥80 years old (OR=1.980; 95% CI: 1.179–3.325; P=0.010), duration of linezolid ≥ 10 days (OR=1.100; 95% CI: 1.050–1.152; P <0.0001), platelet count at baseline (100–149×109/L vs. ≥200×109/L, OR=8.205, 95% CI: 4.419–15.232, P <0.0001; 150–199 ×109/L vs. ≥200×109/L, OR=3.067, 95% CI: 1.676–5.612, P <0.001), leukocyte count at baseline ≥16×109/L (OR=2.580; 95% CI: 1.523–4.373; P <0.0001), creatinine clearance <50 mL/min (OR=2.323; 95% CI: 1.388–3.890; P=0.001), and total protein <60 g/L (OR=1.741; 95% CI: 1.039–2.919; P=0.035) were associated with LAT. The nomogram prediction model called “ADPLCP” (age, duration, platelet, leukocyte, creatinine clearance, protein) was established based on logistic regression. The area under the curve (AUC) of ADPLCP was 0.802 (95% CI: 0.748–0.856; P <0.0001), with 78.9% sensitivity and 69.2% specificity (cut-off was 108). Risk stratification for LAT was performed based on “ADPLCP.” Total points of <100 were defined as low risk, and the possibility of LAT was <32.0%. Total points of 100–150 were defined as medium risk, and the possibility of LAT was 32.0–67.5%. A total point >150 was defined as high risk, and the probability of LAT was >67.5%.
Conclusions
We created the ADPLCP risk score scale to predict the occurrence of LAT in elderly individuals. ADPLCP is simple and feasible and is helpful for the early determination of LAT to guide drug withdrawal or early intervention.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


