Dan Kym, Japsimran Kaur, Nicole Segovia Pham, Eric Klein, Joanna Lind Langner, Ellen Wang, John Schoeneman Vorhies
{"title":"早期手术时间在处理儿科创伤中的有效性。","authors":"Dan Kym, Japsimran Kaur, Nicole Segovia Pham, Eric Klein, Joanna Lind Langner, Ellen Wang, John Schoeneman Vorhies","doi":"10.5312/wjo.v14.i7.516","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The timing of operative treatment for pediatric supracondylar humerus fractures (SCHF) and femoral shaft fractures (FSF) remains controversial. Many fractures previously considered to be surgical emergencies, such as SCHF and open fractures, are now commonly being treated the following day. When presented with an urgent fracture overnight needing operative treatment, the on-call surgeon must choose whether to mobilize resources for a late-night case or to add the case to an elective schedule of the following day.</p><p><strong>Aim: </strong>To describe the effect of a program allowing an early operating room (OR) start for uncomplicated trauma prior to an elective day of surgery to decrease wait times for surgery for urgent fractures admitted overnight.</p><p><strong>Methods: </strong>Starting in October 2017, patients were eligible for the early slot in the OR at the discretion of the surgeon if they were admitted after 21:00 the previous night and before 05:00. We compared demographics and timing of treatment of SCHF and FSF treated one year before and after implementation as well as the survey responses from the surgical team.</p><p><strong>Results: </strong>Of the 44 SCHF meeting inclusion criteria, 16 received treatment before implementation while 28 were treated after. After implementation, the mean wait time for surgery decreased by 4.8 h or 35.4% (13.4 h <i>vs</i> 8.7 h; <i>P</i> = 0.001). There were no significant differences in the operative duration, time in the post anesthesia care unit, and wait time for discharge. Survey results demonstrated decreased popularity of the program among nurses and anesthesiologists relative to surgeons. Whereas 57% of the surgeons believed that the program was effective, only 9% of anesthesiologists and 16% of nurses agreed. The program was ultimately discontinued given the dissatisfaction.</p><p><strong>Conclusion: </strong>Our findings demonstrate significantly reduced wait times for surgery for uncomplicated SCHF presenting overnight while discussing the importance of shared decision-making with the stakeholders. Although the program produced promising results, it also created new conflicts within the OR staff that led to its discontinuation at our institution. Future implementations of such programs should involve stakeholders early in the planning process to better address the needs of the OR staff.</p>","PeriodicalId":47843,"journal":{"name":"World Journal of Orthopedics","volume":"14 7","pages":"516-525"},"PeriodicalIF":2.3000,"publicationDate":"2023-07-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/9c/bd/WJO-14-516.PMC10359751.pdf","citationCount":"0","resultStr":"{\"title\":\"Effectiveness of an early operating room start time in managing pediatric trauma.\",\"authors\":\"Dan Kym, Japsimran Kaur, Nicole Segovia Pham, Eric Klein, Joanna Lind Langner, Ellen Wang, John Schoeneman Vorhies\",\"doi\":\"10.5312/wjo.v14.i7.516\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>The timing of operative treatment for pediatric supracondylar humerus fractures (SCHF) and femoral shaft fractures (FSF) remains controversial. Many fractures previously considered to be surgical emergencies, such as SCHF and open fractures, are now commonly being treated the following day. When presented with an urgent fracture overnight needing operative treatment, the on-call surgeon must choose whether to mobilize resources for a late-night case or to add the case to an elective schedule of the following day.</p><p><strong>Aim: </strong>To describe the effect of a program allowing an early operating room (OR) start for uncomplicated trauma prior to an elective day of surgery to decrease wait times for surgery for urgent fractures admitted overnight.</p><p><strong>Methods: </strong>Starting in October 2017, patients were eligible for the early slot in the OR at the discretion of the surgeon if they were admitted after 21:00 the previous night and before 05:00. We compared demographics and timing of treatment of SCHF and FSF treated one year before and after implementation as well as the survey responses from the surgical team.</p><p><strong>Results: </strong>Of the 44 SCHF meeting inclusion criteria, 16 received treatment before implementation while 28 were treated after. After implementation, the mean wait time for surgery decreased by 4.8 h or 35.4% (13.4 h <i>vs</i> 8.7 h; <i>P</i> = 0.001). There were no significant differences in the operative duration, time in the post anesthesia care unit, and wait time for discharge. Survey results demonstrated decreased popularity of the program among nurses and anesthesiologists relative to surgeons. Whereas 57% of the surgeons believed that the program was effective, only 9% of anesthesiologists and 16% of nurses agreed. The program was ultimately discontinued given the dissatisfaction.</p><p><strong>Conclusion: </strong>Our findings demonstrate significantly reduced wait times for surgery for uncomplicated SCHF presenting overnight while discussing the importance of shared decision-making with the stakeholders. Although the program produced promising results, it also created new conflicts within the OR staff that led to its discontinuation at our institution. Future implementations of such programs should involve stakeholders early in the planning process to better address the needs of the OR staff.</p>\",\"PeriodicalId\":47843,\"journal\":{\"name\":\"World Journal of Orthopedics\",\"volume\":\"14 7\",\"pages\":\"516-525\"},\"PeriodicalIF\":2.3000,\"publicationDate\":\"2023-07-18\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/9c/bd/WJO-14-516.PMC10359751.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"World Journal of Orthopedics\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.5312/wjo.v14.i7.516\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"ORTHOPEDICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"World Journal of Orthopedics","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5312/wjo.v14.i7.516","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"ORTHOPEDICS","Score":null,"Total":0}
Effectiveness of an early operating room start time in managing pediatric trauma.
Background: The timing of operative treatment for pediatric supracondylar humerus fractures (SCHF) and femoral shaft fractures (FSF) remains controversial. Many fractures previously considered to be surgical emergencies, such as SCHF and open fractures, are now commonly being treated the following day. When presented with an urgent fracture overnight needing operative treatment, the on-call surgeon must choose whether to mobilize resources for a late-night case or to add the case to an elective schedule of the following day.
Aim: To describe the effect of a program allowing an early operating room (OR) start for uncomplicated trauma prior to an elective day of surgery to decrease wait times for surgery for urgent fractures admitted overnight.
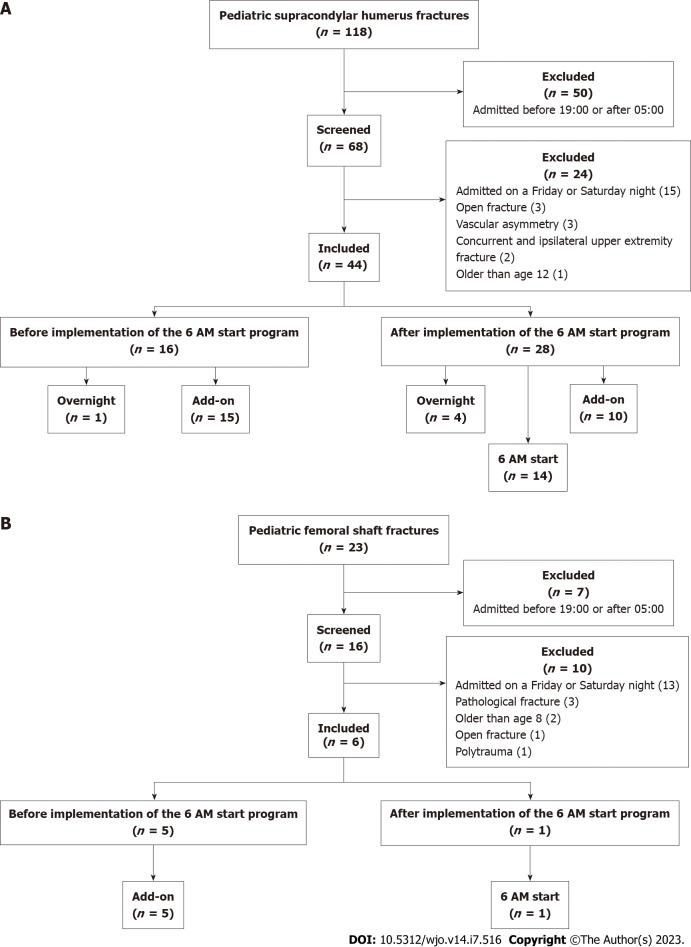
Methods: Starting in October 2017, patients were eligible for the early slot in the OR at the discretion of the surgeon if they were admitted after 21:00 the previous night and before 05:00. We compared demographics and timing of treatment of SCHF and FSF treated one year before and after implementation as well as the survey responses from the surgical team.
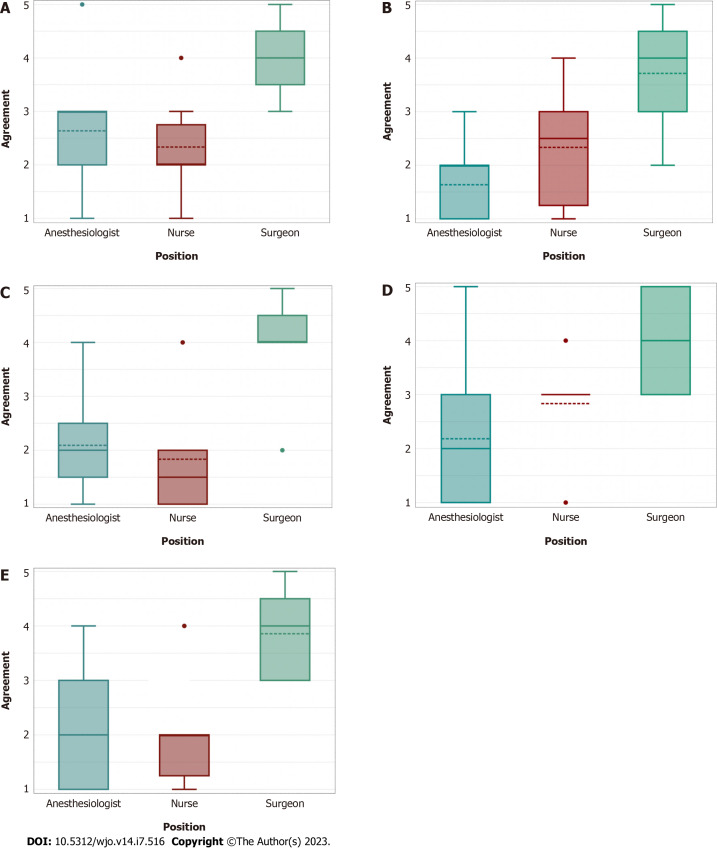
Results: Of the 44 SCHF meeting inclusion criteria, 16 received treatment before implementation while 28 were treated after. After implementation, the mean wait time for surgery decreased by 4.8 h or 35.4% (13.4 h vs 8.7 h; P = 0.001). There were no significant differences in the operative duration, time in the post anesthesia care unit, and wait time for discharge. Survey results demonstrated decreased popularity of the program among nurses and anesthesiologists relative to surgeons. Whereas 57% of the surgeons believed that the program was effective, only 9% of anesthesiologists and 16% of nurses agreed. The program was ultimately discontinued given the dissatisfaction.
Conclusion: Our findings demonstrate significantly reduced wait times for surgery for uncomplicated SCHF presenting overnight while discussing the importance of shared decision-making with the stakeholders. Although the program produced promising results, it also created new conflicts within the OR staff that led to its discontinuation at our institution. Future implementations of such programs should involve stakeholders early in the planning process to better address the needs of the OR staff.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


