{"title":"2017-2019年日本晚期非小细胞肺癌患者的医疗资源利用","authors":"Yasushi Goto MD, PhD , Kodai Kawamura MD, PhD , Tatsuro Fukuhara MD, PhD , Yukiko Namba MD, PhD , Keisuke Aoe MD, PhD , Takehito Shukuya MD, PhD , Takeshi Tsuda MD , Melissa L. Santorelli PhD, MPH , Kazuko Taniguchi MS , Tetsu Kamitani MD, PhD , Masato Irisawa PhD , Kingo Kanda MPharm , Machiko Abe MS , Thomas Burke PharmD, PhD , Hiroshi Nokihara MD, PhD","doi":"10.1016/j.curtheres.2023.100712","DOIUrl":null,"url":null,"abstract":"<div><h3>Background</h3><p>First-line immune checkpoint inhibitor (ICI) monotherapy for advanced non–small cell lung cancer (NSCLC) was introduced in Japan in February 2017. Limited information is available since that time regarding health care resource use for NSCLC in Japan, where the hospitalization burden is high.</p></div><div><h3>Objective</h3><p>We evaluated health care resource use from first- through third-line systemic anticancer therapy for patients with advanced NSCLC included in a multicenter, retrospective chart review study.</p></div><div><h3>Methods</h3><p>Eligible patients were aged 20 years or older with unresectable locally advanced/metastatic NSCLC with no known actionable genomic alteration who initiated first-line systemic anticancer therapy from July 1, 2017, to December 20, 2018, at 23 Japanese hospitals. We calculated the percentage of patients with a record of each resource used, the total number of each resource, and the resource use per 100 patient-weeks of follow-up from initiation of first-, second-, and third-line therapy, overall and by the 3 most common regimen categories, namely, ICI monotherapy, platinum-doublet chemotherapy (without concomitant ICI), and nonplatinum cytotoxic regimens (nonplatinum). Study follow-up ended September 30, 2019.</p></div><div><h3>Results</h3><p>Among 1208 patients (median age = 70 years; 975 [81%] men), 463 patients (38%) received ICI monotherapy, 647 (54%) received platinum-doublet chemotherapy, and 98 (8%) received nonplatinum regimens as first-line therapy. During the study, 621 (51%) patients initiated second-line, and 281 (23%) initiated third-line therapy. The majority of patients experienced ≥1 hospitalization (76%–94%) and ≥1 outpatient visit (85%–90%) during each therapy line. The number of hospitalizations increased from 6.5 per 100 patient-weeks in first-line to 8.0 per 100 patient-weeks in third-line. During first-line therapy, the number of hospitalizations per 100 patient-weeks were 4.8, 8.4, and 6.5 for patients receiving ICI monotherapy, platinum-doublet chemotherapy, and nonplatinum regimens, respectively, and the percentages of hospitalizations categorized as attributable to NSCLC treatment administration (no surgery, procedure, treatment of metastasis, or palliative lung radiation) were 64%, 77%, and 73%, respectively. The number of outpatient visits increased from 43.0 per 100 patient-weeks in first-line to 51.4 per 100 patient-weeks in third-line therapy. During first-line therapy, outpatient visits per 100 patient-weeks were 41.0, 46.7, and 33.0 for patients receiving ICI monotherapy, platinum-doublet chemotherapy, and nonplatinum regimens, respectively, and the percentages of outpatient visits for infusion therapy were 48%, 34%, and 36%, respectively.</p></div><div><h3>Conclusions</h3><p>The results of this study, although solely descriptive, showed differing patterns of health care resource use during first-line therapy among the 3 common systemic anticancer therapy regimens for advanced NSCLC in Japan and suggest that further research is needed to investigate these apparent differences by treatment regimen.</p></div>","PeriodicalId":10920,"journal":{"name":"Current Therapeutic Research-clinical and Experimental","volume":"99 ","pages":"Article 100712"},"PeriodicalIF":1.5000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/b6/8a/main.PMC10372154.pdf","citationCount":"0","resultStr":"{\"title\":\"Health Care Resource Use Among Patients with Advanced Non–Small Cell Lung Cancer in Japan, 2017–2019\",\"authors\":\"Yasushi Goto MD, PhD , Kodai Kawamura MD, PhD , Tatsuro Fukuhara MD, PhD , Yukiko Namba MD, PhD , Keisuke Aoe MD, PhD , Takehito Shukuya MD, PhD , Takeshi Tsuda MD , Melissa L. Santorelli PhD, MPH , Kazuko Taniguchi MS , Tetsu Kamitani MD, PhD , Masato Irisawa PhD , Kingo Kanda MPharm , Machiko Abe MS , Thomas Burke PharmD, PhD , Hiroshi Nokihara MD, PhD\",\"doi\":\"10.1016/j.curtheres.2023.100712\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div><h3>Background</h3><p>First-line immune checkpoint inhibitor (ICI) monotherapy for advanced non–small cell lung cancer (NSCLC) was introduced in Japan in February 2017. Limited information is available since that time regarding health care resource use for NSCLC in Japan, where the hospitalization burden is high.</p></div><div><h3>Objective</h3><p>We evaluated health care resource use from first- through third-line systemic anticancer therapy for patients with advanced NSCLC included in a multicenter, retrospective chart review study.</p></div><div><h3>Methods</h3><p>Eligible patients were aged 20 years or older with unresectable locally advanced/metastatic NSCLC with no known actionable genomic alteration who initiated first-line systemic anticancer therapy from July 1, 2017, to December 20, 2018, at 23 Japanese hospitals. We calculated the percentage of patients with a record of each resource used, the total number of each resource, and the resource use per 100 patient-weeks of follow-up from initiation of first-, second-, and third-line therapy, overall and by the 3 most common regimen categories, namely, ICI monotherapy, platinum-doublet chemotherapy (without concomitant ICI), and nonplatinum cytotoxic regimens (nonplatinum). Study follow-up ended September 30, 2019.</p></div><div><h3>Results</h3><p>Among 1208 patients (median age = 70 years; 975 [81%] men), 463 patients (38%) received ICI monotherapy, 647 (54%) received platinum-doublet chemotherapy, and 98 (8%) received nonplatinum regimens as first-line therapy. During the study, 621 (51%) patients initiated second-line, and 281 (23%) initiated third-line therapy. The majority of patients experienced ≥1 hospitalization (76%–94%) and ≥1 outpatient visit (85%–90%) during each therapy line. The number of hospitalizations increased from 6.5 per 100 patient-weeks in first-line to 8.0 per 100 patient-weeks in third-line. During first-line therapy, the number of hospitalizations per 100 patient-weeks were 4.8, 8.4, and 6.5 for patients receiving ICI monotherapy, platinum-doublet chemotherapy, and nonplatinum regimens, respectively, and the percentages of hospitalizations categorized as attributable to NSCLC treatment administration (no surgery, procedure, treatment of metastasis, or palliative lung radiation) were 64%, 77%, and 73%, respectively. The number of outpatient visits increased from 43.0 per 100 patient-weeks in first-line to 51.4 per 100 patient-weeks in third-line therapy. During first-line therapy, outpatient visits per 100 patient-weeks were 41.0, 46.7, and 33.0 for patients receiving ICI monotherapy, platinum-doublet chemotherapy, and nonplatinum regimens, respectively, and the percentages of outpatient visits for infusion therapy were 48%, 34%, and 36%, respectively.</p></div><div><h3>Conclusions</h3><p>The results of this study, although solely descriptive, showed differing patterns of health care resource use during first-line therapy among the 3 common systemic anticancer therapy regimens for advanced NSCLC in Japan and suggest that further research is needed to investigate these apparent differences by treatment regimen.</p></div>\",\"PeriodicalId\":10920,\"journal\":{\"name\":\"Current Therapeutic Research-clinical and Experimental\",\"volume\":\"99 \",\"pages\":\"Article 100712\"},\"PeriodicalIF\":1.5000,\"publicationDate\":\"2023-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/b6/8a/main.PMC10372154.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Current Therapeutic Research-clinical and Experimental\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://www.sciencedirect.com/science/article/pii/S0011393X23000218\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"MEDICINE, RESEARCH & EXPERIMENTAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Current Therapeutic Research-clinical and Experimental","FirstCategoryId":"1085","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S0011393X23000218","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"MEDICINE, RESEARCH & EXPERIMENTAL","Score":null,"Total":0}
Health Care Resource Use Among Patients with Advanced Non–Small Cell Lung Cancer in Japan, 2017–2019
Background
First-line immune checkpoint inhibitor (ICI) monotherapy for advanced non–small cell lung cancer (NSCLC) was introduced in Japan in February 2017. Limited information is available since that time regarding health care resource use for NSCLC in Japan, where the hospitalization burden is high.
Objective
We evaluated health care resource use from first- through third-line systemic anticancer therapy for patients with advanced NSCLC included in a multicenter, retrospective chart review study.
Methods
Eligible patients were aged 20 years or older with unresectable locally advanced/metastatic NSCLC with no known actionable genomic alteration who initiated first-line systemic anticancer therapy from July 1, 2017, to December 20, 2018, at 23 Japanese hospitals. We calculated the percentage of patients with a record of each resource used, the total number of each resource, and the resource use per 100 patient-weeks of follow-up from initiation of first-, second-, and third-line therapy, overall and by the 3 most common regimen categories, namely, ICI monotherapy, platinum-doublet chemotherapy (without concomitant ICI), and nonplatinum cytotoxic regimens (nonplatinum). Study follow-up ended September 30, 2019.
Results
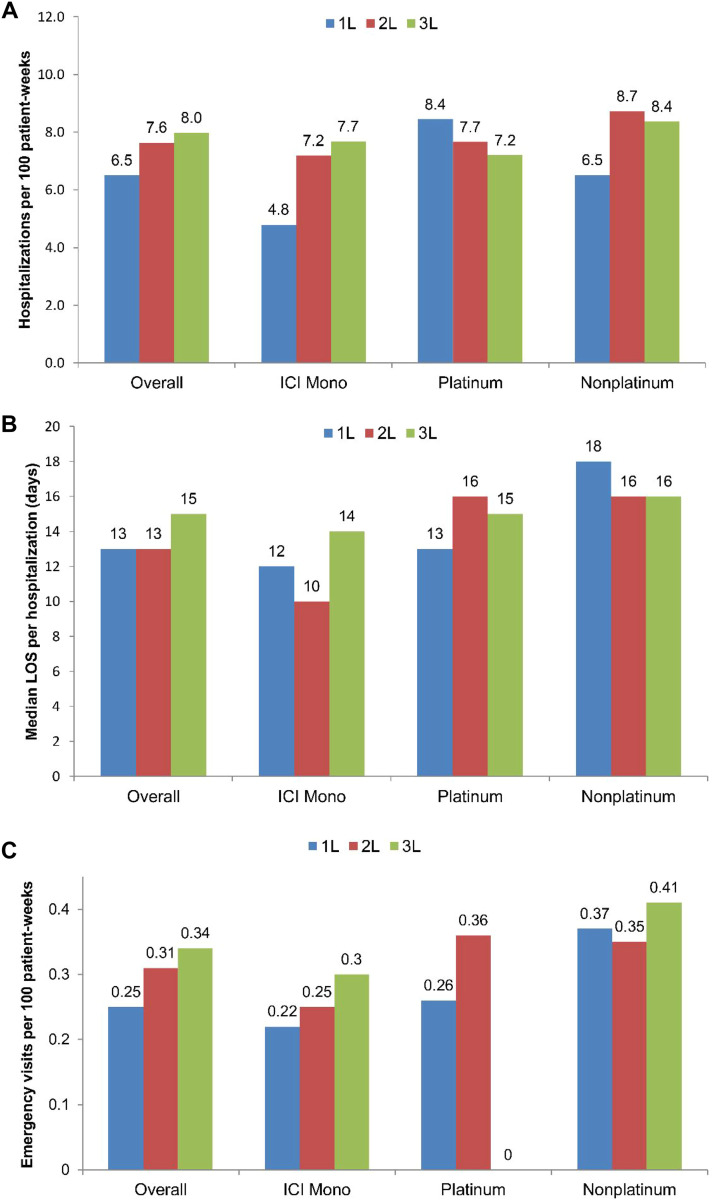
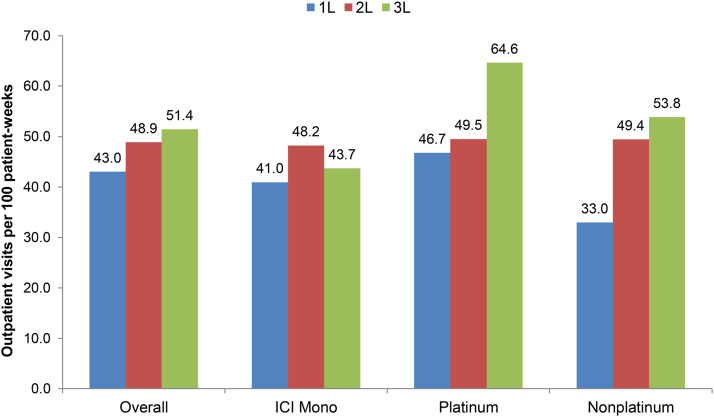
Among 1208 patients (median age = 70 years; 975 [81%] men), 463 patients (38%) received ICI monotherapy, 647 (54%) received platinum-doublet chemotherapy, and 98 (8%) received nonplatinum regimens as first-line therapy. During the study, 621 (51%) patients initiated second-line, and 281 (23%) initiated third-line therapy. The majority of patients experienced ≥1 hospitalization (76%–94%) and ≥1 outpatient visit (85%–90%) during each therapy line. The number of hospitalizations increased from 6.5 per 100 patient-weeks in first-line to 8.0 per 100 patient-weeks in third-line. During first-line therapy, the number of hospitalizations per 100 patient-weeks were 4.8, 8.4, and 6.5 for patients receiving ICI monotherapy, platinum-doublet chemotherapy, and nonplatinum regimens, respectively, and the percentages of hospitalizations categorized as attributable to NSCLC treatment administration (no surgery, procedure, treatment of metastasis, or palliative lung radiation) were 64%, 77%, and 73%, respectively. The number of outpatient visits increased from 43.0 per 100 patient-weeks in first-line to 51.4 per 100 patient-weeks in third-line therapy. During first-line therapy, outpatient visits per 100 patient-weeks were 41.0, 46.7, and 33.0 for patients receiving ICI monotherapy, platinum-doublet chemotherapy, and nonplatinum regimens, respectively, and the percentages of outpatient visits for infusion therapy were 48%, 34%, and 36%, respectively.
Conclusions
The results of this study, although solely descriptive, showed differing patterns of health care resource use during first-line therapy among the 3 common systemic anticancer therapy regimens for advanced NSCLC in Japan and suggest that further research is needed to investigate these apparent differences by treatment regimen.
期刊介绍:
We also encourage the submission of manuscripts presenting preclinical and very preliminary research that may stimulate further investigation of potentially relevant findings, as well as in-depth review articles on specific therapies or disease states, and applied health delivery or pharmacoeconomics.
CTR encourages and supports the submission of manuscripts describing:
• Interventions designed to understand or improve human health, disease treatment or disease prevention;
• Studies that focus on problems that are uncommon in resource-rich countries;
• Research that is "under-published" because of limited access to monetary resources such as English language support and Open Access fees (CTR offers deeply discounted English language editing);
• Republication of articles previously published in non-English journals (eg, evidence-based guidelines) which could be useful if translated into English;
• Preclinical and clinical product development studies that are not pursued for further investigation based upon early phase results.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


