Floris C J Reinders, Peter R S Stijnman, Mischa de Ridder, Patricia A H Doornaert, Cornelis P J Raaijmakers, Marielle E P Philippens
{"title":"头颈部肿瘤放疗患者择期淋巴结的MRI可见性和移位。","authors":"Floris C J Reinders, Peter R S Stijnman, Mischa de Ridder, Patricia A H Doornaert, Cornelis P J Raaijmakers, Marielle E P Philippens","doi":"10.3389/fradi.2022.1033521","DOIUrl":null,"url":null,"abstract":"<p><strong>Background and purpose: </strong>To decrease the impact of radiotherapy to healthy tissues in the head and neck region, we propose to restrict the elective neck irradiation to elective lymph nodes at risk of containing micro metastases instead of the larger lymph node volumes. To assess whether this new concept is achievable in the clinic, we determined the number, volume changes and displacement of elective lymph nodes during the course of radiotherapy.</p><p><strong>Materials and methods: </strong>MRI scans of 10 head and neck cancer (HNC) patients were acquired before radiotherapy and in week 2, 3, 4 and 5 during radiotherapy. The weekly delineations of elective lymph nodes inside the lymph node levels (Ib/II/III/IVa/V) were rigidly registered and analyzed regarding number and volume. The displacement of elective lymph nodes was determined by center of mass (COM) distances, vector-based analysis and the isotropic contour expansion of the lymph nodes of the pre-treatment scan or the scan of the previous week in order to geographically cover 95% of the lymph nodes in the scans of the other weeks.</p><p><strong>Results: </strong>On average, 31 elective lymph nodes in levels Ib-V on each side of the neck were determined. This number remained constant throughout radiotherapy in most lymph node levels. The volume of the elective lymph nodes reduced significantly in all weeks, up to 50% in week 5, compared to the pre-treatment scan. The largest median COM displacements were seen in level V, for example 5.2 mm in week 5 compared to the pre-treatment scan. The displacement of elective lymph nodes was mainly in cranial direction. Geographical coverage was obtained when the lymph node volumes were expanded with 7 mm in case the pre-treatment scan was used and 6.5 mm in case the scan of the previous week was used.</p><p><strong>Conclusion: </strong>Elective lymph nodes of HNC patients remained visible on MRI and decreased in size during radiotherapy. The displacement of elective lymph nodes differ per lymph node level and were mainly directed cranially. Weekly adaptation does not seem to improve coverage of elective lymph nodes. Based on our findings we expect elective lymph node irradiation is achievable in the clinic.</p>","PeriodicalId":73101,"journal":{"name":"Frontiers in radiology","volume":"2 ","pages":"1033521"},"PeriodicalIF":0.0000,"publicationDate":"2022-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10365081/pdf/","citationCount":"1","resultStr":"{\"title\":\"MRI visibility and displacement of elective lymph nodes during radiotherapy in head and neck cancer patients.\",\"authors\":\"Floris C J Reinders, Peter R S Stijnman, Mischa de Ridder, Patricia A H Doornaert, Cornelis P J Raaijmakers, Marielle E P Philippens\",\"doi\":\"10.3389/fradi.2022.1033521\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background and purpose: </strong>To decrease the impact of radiotherapy to healthy tissues in the head and neck region, we propose to restrict the elective neck irradiation to elective lymph nodes at risk of containing micro metastases instead of the larger lymph node volumes. To assess whether this new concept is achievable in the clinic, we determined the number, volume changes and displacement of elective lymph nodes during the course of radiotherapy.</p><p><strong>Materials and methods: </strong>MRI scans of 10 head and neck cancer (HNC) patients were acquired before radiotherapy and in week 2, 3, 4 and 5 during radiotherapy. The weekly delineations of elective lymph nodes inside the lymph node levels (Ib/II/III/IVa/V) were rigidly registered and analyzed regarding number and volume. The displacement of elective lymph nodes was determined by center of mass (COM) distances, vector-based analysis and the isotropic contour expansion of the lymph nodes of the pre-treatment scan or the scan of the previous week in order to geographically cover 95% of the lymph nodes in the scans of the other weeks.</p><p><strong>Results: </strong>On average, 31 elective lymph nodes in levels Ib-V on each side of the neck were determined. This number remained constant throughout radiotherapy in most lymph node levels. The volume of the elective lymph nodes reduced significantly in all weeks, up to 50% in week 5, compared to the pre-treatment scan. The largest median COM displacements were seen in level V, for example 5.2 mm in week 5 compared to the pre-treatment scan. The displacement of elective lymph nodes was mainly in cranial direction. Geographical coverage was obtained when the lymph node volumes were expanded with 7 mm in case the pre-treatment scan was used and 6.5 mm in case the scan of the previous week was used.</p><p><strong>Conclusion: </strong>Elective lymph nodes of HNC patients remained visible on MRI and decreased in size during radiotherapy. The displacement of elective lymph nodes differ per lymph node level and were mainly directed cranially. Weekly adaptation does not seem to improve coverage of elective lymph nodes. Based on our findings we expect elective lymph node irradiation is achievable in the clinic.</p>\",\"PeriodicalId\":73101,\"journal\":{\"name\":\"Frontiers in radiology\",\"volume\":\"2 \",\"pages\":\"1033521\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2022-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10365081/pdf/\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Frontiers in radiology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.3389/fradi.2022.1033521\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Frontiers in radiology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3389/fradi.2022.1033521","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
MRI visibility and displacement of elective lymph nodes during radiotherapy in head and neck cancer patients.
Background and purpose: To decrease the impact of radiotherapy to healthy tissues in the head and neck region, we propose to restrict the elective neck irradiation to elective lymph nodes at risk of containing micro metastases instead of the larger lymph node volumes. To assess whether this new concept is achievable in the clinic, we determined the number, volume changes and displacement of elective lymph nodes during the course of radiotherapy.
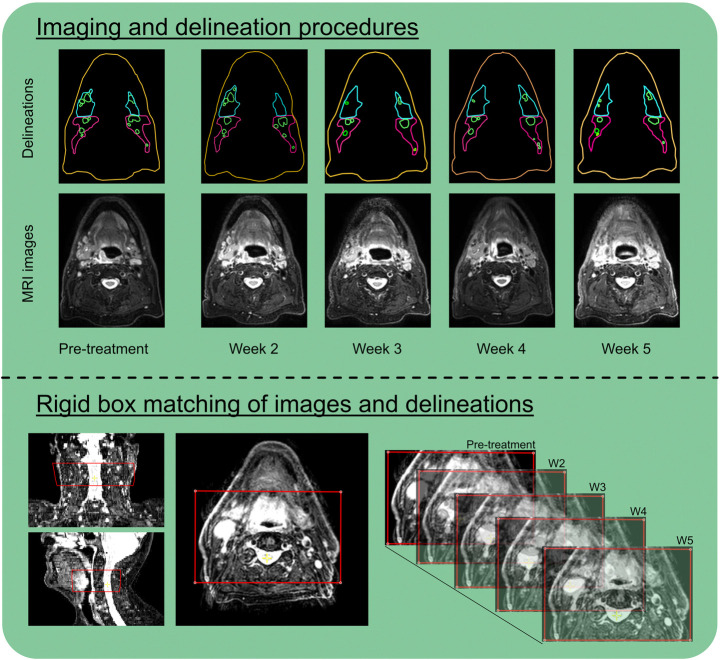
Materials and methods: MRI scans of 10 head and neck cancer (HNC) patients were acquired before radiotherapy and in week 2, 3, 4 and 5 during radiotherapy. The weekly delineations of elective lymph nodes inside the lymph node levels (Ib/II/III/IVa/V) were rigidly registered and analyzed regarding number and volume. The displacement of elective lymph nodes was determined by center of mass (COM) distances, vector-based analysis and the isotropic contour expansion of the lymph nodes of the pre-treatment scan or the scan of the previous week in order to geographically cover 95% of the lymph nodes in the scans of the other weeks.
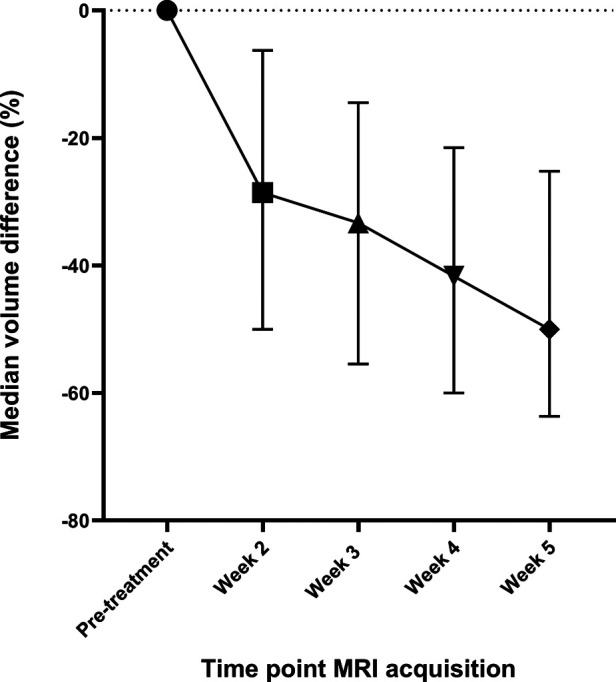
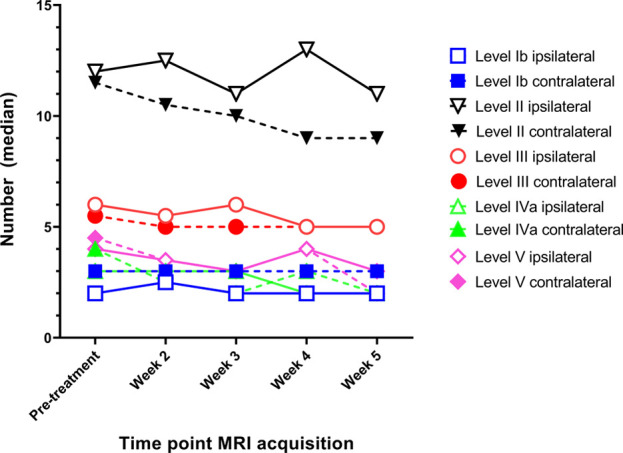
Results: On average, 31 elective lymph nodes in levels Ib-V on each side of the neck were determined. This number remained constant throughout radiotherapy in most lymph node levels. The volume of the elective lymph nodes reduced significantly in all weeks, up to 50% in week 5, compared to the pre-treatment scan. The largest median COM displacements were seen in level V, for example 5.2 mm in week 5 compared to the pre-treatment scan. The displacement of elective lymph nodes was mainly in cranial direction. Geographical coverage was obtained when the lymph node volumes were expanded with 7 mm in case the pre-treatment scan was used and 6.5 mm in case the scan of the previous week was used.
Conclusion: Elective lymph nodes of HNC patients remained visible on MRI and decreased in size during radiotherapy. The displacement of elective lymph nodes differ per lymph node level and were mainly directed cranially. Weekly adaptation does not seem to improve coverage of elective lymph nodes. Based on our findings we expect elective lymph node irradiation is achievable in the clinic.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


