Abigail Funari, Seth S Jeong, Isabella L Pecorari, Isabella Flaquer, Cassidy L Anderson, Vijay Agarwal
{"title":"先前健康垂体的梗死性中风:一个小病例系列和文献回顾。","authors":"Abigail Funari, Seth S Jeong, Isabella L Pecorari, Isabella Flaquer, Cassidy L Anderson, Vijay Agarwal","doi":"10.1055/s-0043-1770788","DOIUrl":null,"url":null,"abstract":"<p><p><b>Introduction</b> We present two cases of suspected pituitary apoplexy found instead to be infarcted pituitary glands without histopathologic evidence of neoplastic cells, likely resulting from spontaneous infarction of previously healthy pituitary glands. <b>Case Presentations</b> The first case is a 55-year-old man who presented with a pulsating headache, nausea, and several months of decreased libido, polyuria, and polydipsia. Magnetic resonance imaging (MRI) revealed a rim-enhancing sellar/suprasellar mass with evidence of recent hemorrhage on the right. Testosterone, follicle-stimulating hormone, and luteinizing hormone levels were suppressed. Analysis of the resected specimen showed fibrocollagenous tissue with evidence of old hemorrhage and microscopic focus of necrotic tissue. The second case is a 56-year-old man who presented with a throbbing headache, associated nausea, and 6 weeks of polyuria and polydipsia. Testosterone levels were found to be low, and 8-hour water deprivation test showed evidence for partial diabetes insipidus. MRI revealed a mass on the right side of the pituitary gland, with evidence of likely hemorrhage on the left. Analysis of the resected specimen showed necrotic tissue without neoplastic cells. <b>Conclusion</b> When evaluating small pituitary lesions in patients presenting with indolent onset of pituitary insufficiency, there should be a high degree of suspicion for an infarcted pituitary gland.</p>","PeriodicalId":44256,"journal":{"name":"Journal of Neurological Surgery Reports","volume":"84 3","pages":"e71-e79"},"PeriodicalIF":0.7000,"publicationDate":"2023-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/2e/67/10-1055-s-0043-1770788.PMC10365896.pdf","citationCount":"1","resultStr":"{\"title\":\"Infarctive Apoplexy of Previously Healthy Pituitary Glands: A Small Case Series and Literature Review.\",\"authors\":\"Abigail Funari, Seth S Jeong, Isabella L Pecorari, Isabella Flaquer, Cassidy L Anderson, Vijay Agarwal\",\"doi\":\"10.1055/s-0043-1770788\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p><b>Introduction</b> We present two cases of suspected pituitary apoplexy found instead to be infarcted pituitary glands without histopathologic evidence of neoplastic cells, likely resulting from spontaneous infarction of previously healthy pituitary glands. <b>Case Presentations</b> The first case is a 55-year-old man who presented with a pulsating headache, nausea, and several months of decreased libido, polyuria, and polydipsia. Magnetic resonance imaging (MRI) revealed a rim-enhancing sellar/suprasellar mass with evidence of recent hemorrhage on the right. Testosterone, follicle-stimulating hormone, and luteinizing hormone levels were suppressed. Analysis of the resected specimen showed fibrocollagenous tissue with evidence of old hemorrhage and microscopic focus of necrotic tissue. The second case is a 56-year-old man who presented with a throbbing headache, associated nausea, and 6 weeks of polyuria and polydipsia. Testosterone levels were found to be low, and 8-hour water deprivation test showed evidence for partial diabetes insipidus. MRI revealed a mass on the right side of the pituitary gland, with evidence of likely hemorrhage on the left. Analysis of the resected specimen showed necrotic tissue without neoplastic cells. <b>Conclusion</b> When evaluating small pituitary lesions in patients presenting with indolent onset of pituitary insufficiency, there should be a high degree of suspicion for an infarcted pituitary gland.</p>\",\"PeriodicalId\":44256,\"journal\":{\"name\":\"Journal of Neurological Surgery Reports\",\"volume\":\"84 3\",\"pages\":\"e71-e79\"},\"PeriodicalIF\":0.7000,\"publicationDate\":\"2023-07-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/2e/67/10-1055-s-0043-1770788.PMC10365896.pdf\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Neurological Surgery Reports\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1055/s-0043-1770788\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q4\",\"JCRName\":\"CLINICAL NEUROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Neurological Surgery Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1055/s-0043-1770788","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
Infarctive Apoplexy of Previously Healthy Pituitary Glands: A Small Case Series and Literature Review.
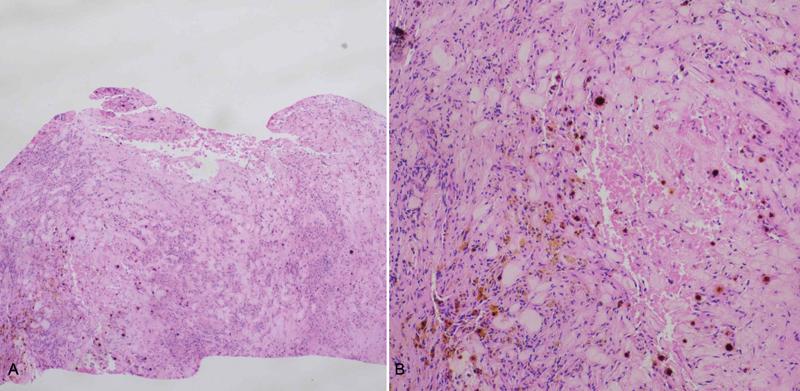
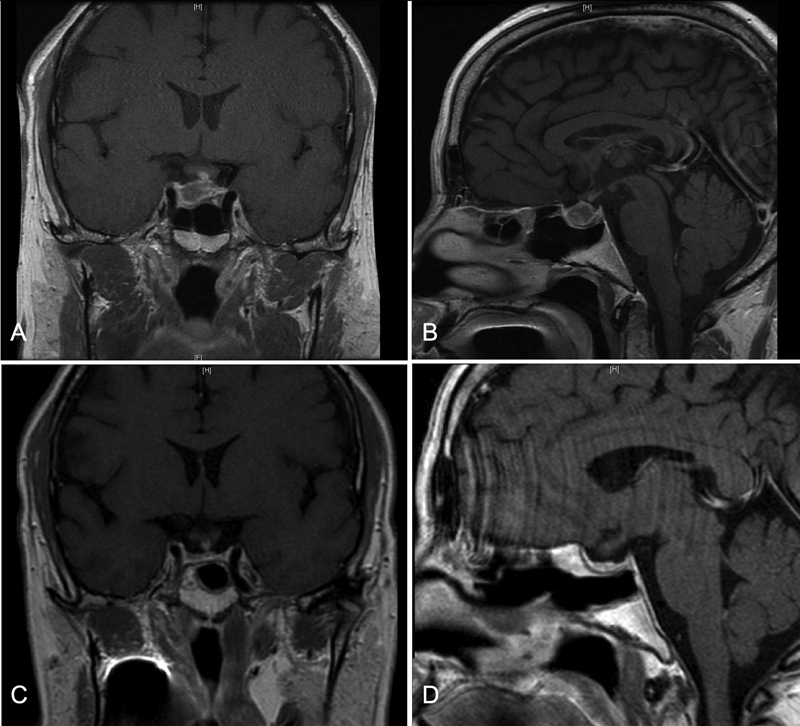
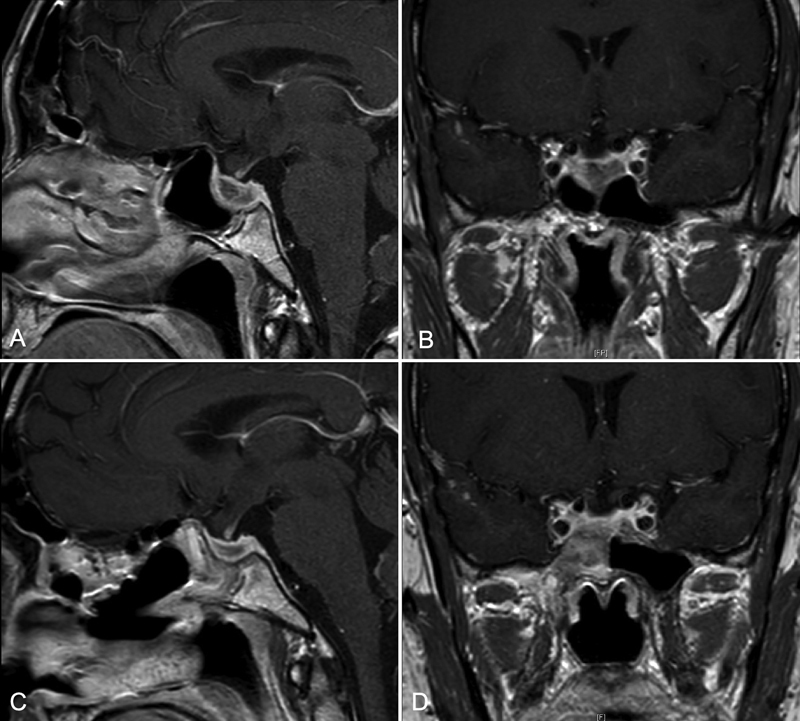
Introduction We present two cases of suspected pituitary apoplexy found instead to be infarcted pituitary glands without histopathologic evidence of neoplastic cells, likely resulting from spontaneous infarction of previously healthy pituitary glands. Case Presentations The first case is a 55-year-old man who presented with a pulsating headache, nausea, and several months of decreased libido, polyuria, and polydipsia. Magnetic resonance imaging (MRI) revealed a rim-enhancing sellar/suprasellar mass with evidence of recent hemorrhage on the right. Testosterone, follicle-stimulating hormone, and luteinizing hormone levels were suppressed. Analysis of the resected specimen showed fibrocollagenous tissue with evidence of old hemorrhage and microscopic focus of necrotic tissue. The second case is a 56-year-old man who presented with a throbbing headache, associated nausea, and 6 weeks of polyuria and polydipsia. Testosterone levels were found to be low, and 8-hour water deprivation test showed evidence for partial diabetes insipidus. MRI revealed a mass on the right side of the pituitary gland, with evidence of likely hemorrhage on the left. Analysis of the resected specimen showed necrotic tissue without neoplastic cells. Conclusion When evaluating small pituitary lesions in patients presenting with indolent onset of pituitary insufficiency, there should be a high degree of suspicion for an infarcted pituitary gland.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


