{"title":"紧急ABO血型不合的活体肝移植治疗Wilson病引起的急性肝衰竭。","authors":"Joseph J Valamparampil, Deepti Sachan, Naresh Shanmugam, Srinivas Mettu Reddy, Mohamed Rela","doi":"10.4103/ajts.ajts_55_21","DOIUrl":null,"url":null,"abstract":"<p><p>We report the clinical outcome of an emergency ABO incompatible-liver transplantation (LT) for an 8-year-old child with Wilson's disease-induced acute liver failure. The pretransplant anti-A antibody titer was 1:64, and hence he underwent three cycles of conventional plasma exchange as pretransplant liver supportive treatment for deranged coagulopathy and liver function followed by one cycle of immunoadsorption (IA) prior to LT. The posttransplant immunosuppression consisted of rituximab, tacrolimus, mycophenolate mofetil, and corticosteroid. The patient had anti-A isoagglutinin rebound with elevated aminotransferases levels from postoperative day 7 for which he was restarted on IA plasmapheresis, but antibody titers did not decrease. Hence, he was switched to conventional plasmapheresis (CP) with which anti-A antibody titers decreased. The total dose of rituximab (150 milligrams/square meter of body surface area) was given in two divided doses of 75 mg at D-1 and D + 8 which was much less than the dose conventionally advocated (375 milligrams/square meter of body surface area). He is clinically well with good graft function without rejection after 1 year of follow-up. This case illustrates that IA and CP in conjunction with adequate immunosuppression is a viable approach in emergency ABO-incompatible-LT in Wilson disease-induced acute liver failure.</p>","PeriodicalId":42296,"journal":{"name":"Asian Journal of Transfusion Science","volume":"17 1","pages":"128-130"},"PeriodicalIF":0.6000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/02/87/AJTS-17-128.PMC10180780.pdf","citationCount":"0","resultStr":"{\"title\":\"Emergency ABO-incompatible living donor liver transplantation in Wilson disease-induced acute liver failure.\",\"authors\":\"Joseph J Valamparampil, Deepti Sachan, Naresh Shanmugam, Srinivas Mettu Reddy, Mohamed Rela\",\"doi\":\"10.4103/ajts.ajts_55_21\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>We report the clinical outcome of an emergency ABO incompatible-liver transplantation (LT) for an 8-year-old child with Wilson's disease-induced acute liver failure. The pretransplant anti-A antibody titer was 1:64, and hence he underwent three cycles of conventional plasma exchange as pretransplant liver supportive treatment for deranged coagulopathy and liver function followed by one cycle of immunoadsorption (IA) prior to LT. The posttransplant immunosuppression consisted of rituximab, tacrolimus, mycophenolate mofetil, and corticosteroid. The patient had anti-A isoagglutinin rebound with elevated aminotransferases levels from postoperative day 7 for which he was restarted on IA plasmapheresis, but antibody titers did not decrease. Hence, he was switched to conventional plasmapheresis (CP) with which anti-A antibody titers decreased. The total dose of rituximab (150 milligrams/square meter of body surface area) was given in two divided doses of 75 mg at D-1 and D + 8 which was much less than the dose conventionally advocated (375 milligrams/square meter of body surface area). He is clinically well with good graft function without rejection after 1 year of follow-up. This case illustrates that IA and CP in conjunction with adequate immunosuppression is a viable approach in emergency ABO-incompatible-LT in Wilson disease-induced acute liver failure.</p>\",\"PeriodicalId\":42296,\"journal\":{\"name\":\"Asian Journal of Transfusion Science\",\"volume\":\"17 1\",\"pages\":\"128-130\"},\"PeriodicalIF\":0.6000,\"publicationDate\":\"2023-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/02/87/AJTS-17-128.PMC10180780.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Asian Journal of Transfusion Science\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.4103/ajts.ajts_55_21\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2022/5/26 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q4\",\"JCRName\":\"HEMATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Asian Journal of Transfusion Science","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4103/ajts.ajts_55_21","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/5/26 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"HEMATOLOGY","Score":null,"Total":0}
Emergency ABO-incompatible living donor liver transplantation in Wilson disease-induced acute liver failure.
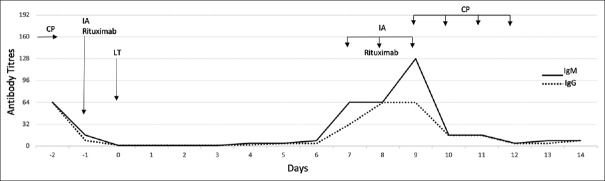
We report the clinical outcome of an emergency ABO incompatible-liver transplantation (LT) for an 8-year-old child with Wilson's disease-induced acute liver failure. The pretransplant anti-A antibody titer was 1:64, and hence he underwent three cycles of conventional plasma exchange as pretransplant liver supportive treatment for deranged coagulopathy and liver function followed by one cycle of immunoadsorption (IA) prior to LT. The posttransplant immunosuppression consisted of rituximab, tacrolimus, mycophenolate mofetil, and corticosteroid. The patient had anti-A isoagglutinin rebound with elevated aminotransferases levels from postoperative day 7 for which he was restarted on IA plasmapheresis, but antibody titers did not decrease. Hence, he was switched to conventional plasmapheresis (CP) with which anti-A antibody titers decreased. The total dose of rituximab (150 milligrams/square meter of body surface area) was given in two divided doses of 75 mg at D-1 and D + 8 which was much less than the dose conventionally advocated (375 milligrams/square meter of body surface area). He is clinically well with good graft function without rejection after 1 year of follow-up. This case illustrates that IA and CP in conjunction with adequate immunosuppression is a viable approach in emergency ABO-incompatible-LT in Wilson disease-induced acute liver failure.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


