{"title":"MELAS卒中样发作的临床放射学诊断标准。","authors":"Vadim Khasminsky, Eitan Auriel, Judith Luckman, Ruth Eliahou, Edna Inbar, Keshet Pardo, Yuval Landau, Rani Barnea, Maor Mermelstein, Shahar Shelly, Jonathan Naftali, Shlomi Peretz","doi":"10.1212/NXG.0000000000200082","DOIUrl":null,"url":null,"abstract":"<p><strong>Background and objectives: </strong>Stroke-like episodes (SLEs) in patients with mitochondrial encephalomyopathy, lactic acidosis, and stroke-like episodes (MELAS) syndrome are often misdiagnosed as acute ischemic stroke (AIS). We aimed to determine unique clinical and neuroimaging features for SLEs and formulate diagnostic criteria.</p><p><strong>Methods: </strong>We retrospectively identified patients with MELAS admitted for SLEs between January 2012 and December 2021. Clinical features and imaging findings were compared with a cohort of patients who presented with AIS and similar lesion topography. A set of criteria was formulated and then tested by a blinded rater to evaluate diagnostic performance.</p><p><strong>Results: </strong>Eleven MELAS patients with 17 SLE and 21 AISs were included. Patients with SLEs were younger (median 45 [37-60] vs 77 [68-82] years, <i>p</i> < 0.01) and had a lower body mass index (18 ± 2.6 vs 29 ± 4, <i>p</i> < 0.01), more commonly reported hearing loss (91% vs 5%, <i>p</i> < 0.01), and more commonly presented with headache and/or seizures (41% vs 0%, <i>p</i> < 0.01). The earliest neuroimaging test performed at presentation was uniformly a noncontrast CT. Two main patterns of lesion topography with a stereotypical spatiotemporal evolution were identified-an anterior pattern (7/21, 41%) starting at the temporal operculum and spreading to the peripheral frontal cortex and a posterior pattern (10/21, 59%) starting at the cuneus/precuneus and spreading to the lateral occipital and parietal cortex. Other distinguishing features for SLEs vs AIS were cerebellar atrophy (91% vs 19%, <i>p</i> < 0.01), previous cortical lesions with typical SLE distribution (46% vs 9%, <i>p</i> = 0.03), acute lesion tissue hyperemia and venous engorgement on CT angiography (CTA) (45% vs 0%, <i>p</i> < 0.01), and no large vessel occlusion on CTA (0% vs 100%, <i>p</i> < 0.01). Based on these clinicoradiologic features, a set of diagnostic criteria were constructed for possible SLE (sensitivity 100%, specificity 81%, AUC 0.905) and probable SLE (sensitivity 88%, specificity 95%, AUC 0.917).</p><p><strong>Discussion: </strong>Clinicoradiologic criteria based on simple anamnesis and a CT scan at presentation can accurately diagnose SLE and lead to early administration of appropriate therapy.</p><p><strong>Classification of evidence: </strong>This study provides Class III evidence that an algorithm using clinical and imaging features can differentiate stroke-like episodes due to MELAS from acute ischemic strokes.</p>","PeriodicalId":48613,"journal":{"name":"Neurology-Genetics","volume":"9 4","pages":"e200082"},"PeriodicalIF":3.0000,"publicationDate":"2023-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/5d/96/NXG-2023-000024.PMC10323819.pdf","citationCount":"0","resultStr":"{\"title\":\"Clinicoradiologic Criteria for the Diagnosis of Stroke-like Episodes in MELAS.\",\"authors\":\"Vadim Khasminsky, Eitan Auriel, Judith Luckman, Ruth Eliahou, Edna Inbar, Keshet Pardo, Yuval Landau, Rani Barnea, Maor Mermelstein, Shahar Shelly, Jonathan Naftali, Shlomi Peretz\",\"doi\":\"10.1212/NXG.0000000000200082\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background and objectives: </strong>Stroke-like episodes (SLEs) in patients with mitochondrial encephalomyopathy, lactic acidosis, and stroke-like episodes (MELAS) syndrome are often misdiagnosed as acute ischemic stroke (AIS). We aimed to determine unique clinical and neuroimaging features for SLEs and formulate diagnostic criteria.</p><p><strong>Methods: </strong>We retrospectively identified patients with MELAS admitted for SLEs between January 2012 and December 2021. Clinical features and imaging findings were compared with a cohort of patients who presented with AIS and similar lesion topography. A set of criteria was formulated and then tested by a blinded rater to evaluate diagnostic performance.</p><p><strong>Results: </strong>Eleven MELAS patients with 17 SLE and 21 AISs were included. Patients with SLEs were younger (median 45 [37-60] vs 77 [68-82] years, <i>p</i> < 0.01) and had a lower body mass index (18 ± 2.6 vs 29 ± 4, <i>p</i> < 0.01), more commonly reported hearing loss (91% vs 5%, <i>p</i> < 0.01), and more commonly presented with headache and/or seizures (41% vs 0%, <i>p</i> < 0.01). The earliest neuroimaging test performed at presentation was uniformly a noncontrast CT. Two main patterns of lesion topography with a stereotypical spatiotemporal evolution were identified-an anterior pattern (7/21, 41%) starting at the temporal operculum and spreading to the peripheral frontal cortex and a posterior pattern (10/21, 59%) starting at the cuneus/precuneus and spreading to the lateral occipital and parietal cortex. Other distinguishing features for SLEs vs AIS were cerebellar atrophy (91% vs 19%, <i>p</i> < 0.01), previous cortical lesions with typical SLE distribution (46% vs 9%, <i>p</i> = 0.03), acute lesion tissue hyperemia and venous engorgement on CT angiography (CTA) (45% vs 0%, <i>p</i> < 0.01), and no large vessel occlusion on CTA (0% vs 100%, <i>p</i> < 0.01). Based on these clinicoradiologic features, a set of diagnostic criteria were constructed for possible SLE (sensitivity 100%, specificity 81%, AUC 0.905) and probable SLE (sensitivity 88%, specificity 95%, AUC 0.917).</p><p><strong>Discussion: </strong>Clinicoradiologic criteria based on simple anamnesis and a CT scan at presentation can accurately diagnose SLE and lead to early administration of appropriate therapy.</p><p><strong>Classification of evidence: </strong>This study provides Class III evidence that an algorithm using clinical and imaging features can differentiate stroke-like episodes due to MELAS from acute ischemic strokes.</p>\",\"PeriodicalId\":48613,\"journal\":{\"name\":\"Neurology-Genetics\",\"volume\":\"9 4\",\"pages\":\"e200082\"},\"PeriodicalIF\":3.0000,\"publicationDate\":\"2023-08-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/5d/96/NXG-2023-000024.PMC10323819.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Neurology-Genetics\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1212/NXG.0000000000200082\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"CLINICAL NEUROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Neurology-Genetics","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1212/NXG.0000000000200082","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
摘要
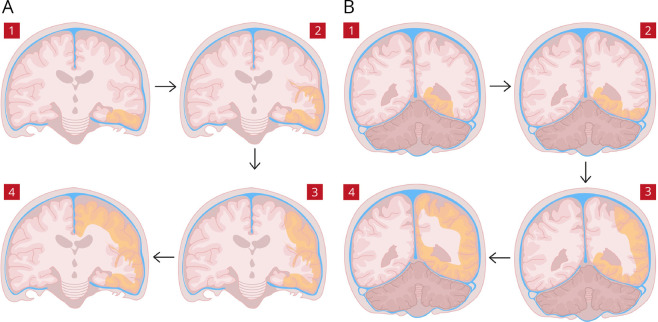
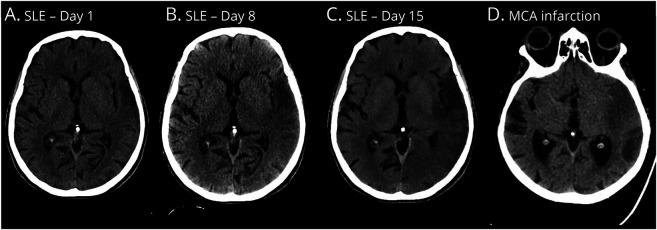
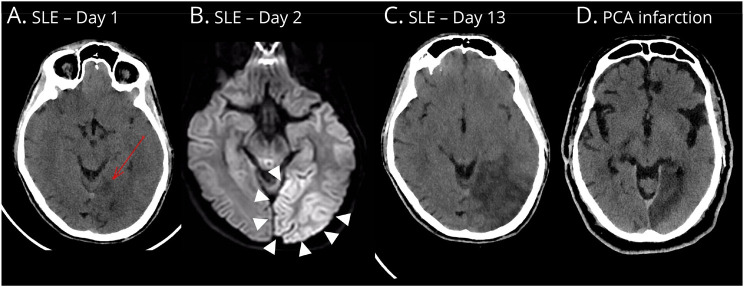
背景和目的:线粒体脑肌病、乳酸酸中毒和卒中样发作(MELAS)综合征患者的卒中样发作(SLEs)常被误诊为急性缺血性卒中(AIS)。我们的目的是确定独特的临床和神经影像学特征的SLEs和制定诊断标准。方法:回顾性分析2012年1月至2021年12月期间因SLEs入院的MELAS患者。将临床特征和影像学结果与一组表现为AIS和类似病变地形的患者进行比较。制定了一套标准,然后由盲法评分者进行测试,以评估诊断性能。结果:11例MELAS患者合并17例SLE和21例ais。SLEs患者较年轻(中位年龄为45岁[37-60]vs 77岁[68-82],p < 0.01),体重指数较低(18±2.6 vs 29±4,p < 0.01),更常见的报告听力损失(91% vs 5%, p < 0.01),更常见的表现为头痛和/或癫痫发作(41% vs 0%, p < 0.01)。在发病时进行的最早的神经影像学检查均为非对比CT。发现两种主要的病变形态具有典型的时空演化特征:从颞盖开始向外周额叶皮层扩散的前型(7/ 21,41 %)和从楔叶/楔前叶开始向外侧枕叶和顶叶皮层扩散的后型(10/ 21,59 %)。SLE与AIS的其他区别特征是小脑萎缩(91% vs 19%, p < 0.01),既往皮质病变具有典型SLE分布(46% vs 9%, p = 0.03),急性病变组织充血和CT血管造影(CTA)静脉充血(45% vs 0%, p < 0.01), CTA无大血管闭塞(0% vs 100%, p < 0.01)。基于这些临床放射学特征,构建了一套可能SLE(敏感性100%,特异性81%,AUC 0.905)和可能SLE(敏感性88%,特异性95%,AUC 0.917)的诊断标准。讨论:基于简单记忆的临床放射学标准和表现时的CT扫描可以准确诊断SLE并导致早期给予适当治疗。证据分类:本研究提供了III类证据,表明一种基于临床和影像学特征的算法可以区分MELAS引起的卒中样发作和急性缺血性卒中。
Clinicoradiologic Criteria for the Diagnosis of Stroke-like Episodes in MELAS.
Background and objectives: Stroke-like episodes (SLEs) in patients with mitochondrial encephalomyopathy, lactic acidosis, and stroke-like episodes (MELAS) syndrome are often misdiagnosed as acute ischemic stroke (AIS). We aimed to determine unique clinical and neuroimaging features for SLEs and formulate diagnostic criteria.
Methods: We retrospectively identified patients with MELAS admitted for SLEs between January 2012 and December 2021. Clinical features and imaging findings were compared with a cohort of patients who presented with AIS and similar lesion topography. A set of criteria was formulated and then tested by a blinded rater to evaluate diagnostic performance.
Results: Eleven MELAS patients with 17 SLE and 21 AISs were included. Patients with SLEs were younger (median 45 [37-60] vs 77 [68-82] years, p < 0.01) and had a lower body mass index (18 ± 2.6 vs 29 ± 4, p < 0.01), more commonly reported hearing loss (91% vs 5%, p < 0.01), and more commonly presented with headache and/or seizures (41% vs 0%, p < 0.01). The earliest neuroimaging test performed at presentation was uniformly a noncontrast CT. Two main patterns of lesion topography with a stereotypical spatiotemporal evolution were identified-an anterior pattern (7/21, 41%) starting at the temporal operculum and spreading to the peripheral frontal cortex and a posterior pattern (10/21, 59%) starting at the cuneus/precuneus and spreading to the lateral occipital and parietal cortex. Other distinguishing features for SLEs vs AIS were cerebellar atrophy (91% vs 19%, p < 0.01), previous cortical lesions with typical SLE distribution (46% vs 9%, p = 0.03), acute lesion tissue hyperemia and venous engorgement on CT angiography (CTA) (45% vs 0%, p < 0.01), and no large vessel occlusion on CTA (0% vs 100%, p < 0.01). Based on these clinicoradiologic features, a set of diagnostic criteria were constructed for possible SLE (sensitivity 100%, specificity 81%, AUC 0.905) and probable SLE (sensitivity 88%, specificity 95%, AUC 0.917).
Discussion: Clinicoradiologic criteria based on simple anamnesis and a CT scan at presentation can accurately diagnose SLE and lead to early administration of appropriate therapy.
Classification of evidence: This study provides Class III evidence that an algorithm using clinical and imaging features can differentiate stroke-like episodes due to MELAS from acute ischemic strokes.
期刊介绍:
Neurology: Genetics is an online open access journal publishing peer-reviewed reports in the field of neurogenetics. Original articles in all areas of neurogenetics will be published including rare and common genetic variation, genotype-phenotype correlations, outlier phenotypes as a result of mutations in known disease-genes, and genetic variations with a putative link to diseases. This will include studies reporting on genetic disease risk and pharmacogenomics. In addition, Neurology: Genetics will publish results of gene-based clinical trials (viral, ASO, etc.). Genetically engineered model systems are not a primary focus of Neurology: Genetics, but studies using model systems for treatment trials are welcome, including well-powered studies reporting negative results.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


