Nancy Herrera-Leaño, Julián E Barahona-Correa, Oscar Muñoz-Velandia, Daniel G Fernández-Ávila, Alejandro Mariño-Correa, Ángel Alberto García
{"title":"评估心力衰竭诊所对晚期心力衰竭患者静脉注射呋塞米的利尿效果。","authors":"Nancy Herrera-Leaño, Julián E Barahona-Correa, Oscar Muñoz-Velandia, Daniel G Fernández-Ávila, Alejandro Mariño-Correa, Ángel Alberto García","doi":"10.1177/17539447231184984","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Diuretic efficiency (DE) is an independent predictor of all-cause mortality in acute heart failure (HF) at long-term follow-up. The performance of DE in advanced HF and the outpatient scenario is unclear.</p><p><strong>Methods: </strong>Survival function analysis on a retrospective cohort of patients with advanced HF followed at the outpatient clinic of Hospital Universitario San Ignacio (Bogotá, Colombia) between 2017 and 2021. DE was calculated as the average of total diuresis in milliliters divided by the dose of IV furosemide in milligrams for each 6-h session, considering all the sessions in which the patient received levosimendan and IV furosemide. We stratified DE in high or low using the median value of the cohort as the cutoff value. The primary outcome was a composite of all-cause mortality and HF hospitalizations during a 12-month follow-up. Kaplan-Meier curves and log-rank test were used to compare patients with high and low DE.</p><p><strong>Results: </strong>In all, 41 patients (66.5 ± 13.2 years old, 75.6% men) were included in the study, with a median DE of 24.5 mL/mg. In total, 20 patients were categorized as low and 21 as high DE. The composite outcome occurred more often in the high DE group (13 <i>versus</i> 5, log-rank test <i>p</i> = 0.0385); the all-cause mortality rate was 29.2% and was more frequent in the high DE group (11 <i>versus</i> 1, log-rank test <i>p</i> = 0.0026).</p><p><strong>Conclusion: </strong>In patients with advanced HF on intermittent inotropic therapy, a high DE efficiency is associated with a higher risk of mortality or HF hospitalization in a 12-month follow-up period.</p>","PeriodicalId":23035,"journal":{"name":"Therapeutic Advances in Cardiovascular Disease","volume":"17 ","pages":"17539447231184984"},"PeriodicalIF":2.2000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/a7/5e/10.1177_17539447231184984.PMC10331187.pdf","citationCount":"0","resultStr":"{\"title\":\"Evaluation of diuretic efficiency of intravenous furosemide in patients with advanced heart failure in a heart failure clinic.\",\"authors\":\"Nancy Herrera-Leaño, Julián E Barahona-Correa, Oscar Muñoz-Velandia, Daniel G Fernández-Ávila, Alejandro Mariño-Correa, Ángel Alberto García\",\"doi\":\"10.1177/17539447231184984\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Diuretic efficiency (DE) is an independent predictor of all-cause mortality in acute heart failure (HF) at long-term follow-up. The performance of DE in advanced HF and the outpatient scenario is unclear.</p><p><strong>Methods: </strong>Survival function analysis on a retrospective cohort of patients with advanced HF followed at the outpatient clinic of Hospital Universitario San Ignacio (Bogotá, Colombia) between 2017 and 2021. DE was calculated as the average of total diuresis in milliliters divided by the dose of IV furosemide in milligrams for each 6-h session, considering all the sessions in which the patient received levosimendan and IV furosemide. We stratified DE in high or low using the median value of the cohort as the cutoff value. The primary outcome was a composite of all-cause mortality and HF hospitalizations during a 12-month follow-up. Kaplan-Meier curves and log-rank test were used to compare patients with high and low DE.</p><p><strong>Results: </strong>In all, 41 patients (66.5 ± 13.2 years old, 75.6% men) were included in the study, with a median DE of 24.5 mL/mg. In total, 20 patients were categorized as low and 21 as high DE. The composite outcome occurred more often in the high DE group (13 <i>versus</i> 5, log-rank test <i>p</i> = 0.0385); the all-cause mortality rate was 29.2% and was more frequent in the high DE group (11 <i>versus</i> 1, log-rank test <i>p</i> = 0.0026).</p><p><strong>Conclusion: </strong>In patients with advanced HF on intermittent inotropic therapy, a high DE efficiency is associated with a higher risk of mortality or HF hospitalization in a 12-month follow-up period.</p>\",\"PeriodicalId\":23035,\"journal\":{\"name\":\"Therapeutic Advances in Cardiovascular Disease\",\"volume\":\"17 \",\"pages\":\"17539447231184984\"},\"PeriodicalIF\":2.2000,\"publicationDate\":\"2023-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/a7/5e/10.1177_17539447231184984.PMC10331187.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Therapeutic Advances in Cardiovascular Disease\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1177/17539447231184984\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Therapeutic Advances in Cardiovascular Disease","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/17539447231184984","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
摘要
简介在长期随访中,利尿剂效率(DE)是急性心力衰竭(HF)患者全因死亡率的独立预测指标。在晚期心力衰竭和门诊情况下,利尿效率的表现尚不明确:对2017年至2021年间在圣伊格纳西奥大学医院(哥伦比亚波哥大)门诊随访的晚期心力衰竭患者进行回顾性队列生存功能分析。考虑到患者接受左西孟旦和呋塞米静脉注射的所有疗程,以毫升为单位的总利尿量除以以毫克为单位的静脉注射呋塞米剂量的平均值来计算患者的生存率。我们以队列的中位值作为分界值,将 DE 分为高或低。主要结果是随访 12 个月期间的全因死亡率和心房颤动住院率的复合值。采用卡普兰-梅耶曲线和对数秩检验对高 DE 和低 DE 患者进行比较:研究共纳入 41 名患者(66.5 ± 13.2 岁,75.6% 为男性),中位 DE 为 24.5 mL/mg。共有 20 名患者被归类为低密度脂蛋白血症,21 名患者被归类为高密度脂蛋白血症。高密度脂蛋白血症组的综合结果发生率更高(13 对 5,对数秩检验 p = 0.0385);全因死亡率为 29.2%,高密度脂蛋白血症组的发生率更高(11 对 1,对数秩检验 p = 0.0026):结论:在接受间歇性肌力治疗的晚期心房颤动患者中,高去氧效率与12个月随访期间较高的死亡或心房颤动住院风险相关。
Evaluation of diuretic efficiency of intravenous furosemide in patients with advanced heart failure in a heart failure clinic.
Introduction: Diuretic efficiency (DE) is an independent predictor of all-cause mortality in acute heart failure (HF) at long-term follow-up. The performance of DE in advanced HF and the outpatient scenario is unclear.
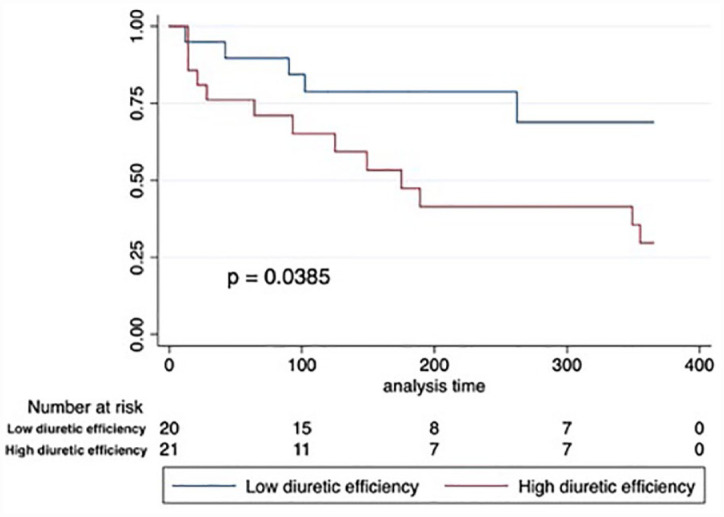
Methods: Survival function analysis on a retrospective cohort of patients with advanced HF followed at the outpatient clinic of Hospital Universitario San Ignacio (Bogotá, Colombia) between 2017 and 2021. DE was calculated as the average of total diuresis in milliliters divided by the dose of IV furosemide in milligrams for each 6-h session, considering all the sessions in which the patient received levosimendan and IV furosemide. We stratified DE in high or low using the median value of the cohort as the cutoff value. The primary outcome was a composite of all-cause mortality and HF hospitalizations during a 12-month follow-up. Kaplan-Meier curves and log-rank test were used to compare patients with high and low DE.
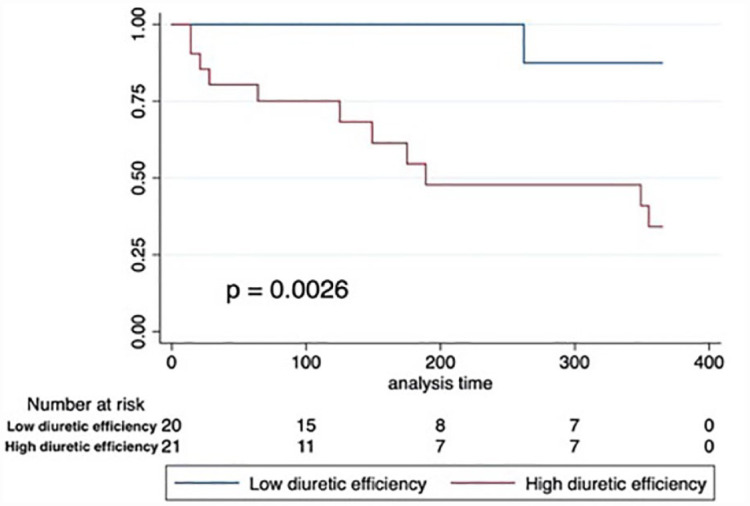
Results: In all, 41 patients (66.5 ± 13.2 years old, 75.6% men) were included in the study, with a median DE of 24.5 mL/mg. In total, 20 patients were categorized as low and 21 as high DE. The composite outcome occurred more often in the high DE group (13 versus 5, log-rank test p = 0.0385); the all-cause mortality rate was 29.2% and was more frequent in the high DE group (11 versus 1, log-rank test p = 0.0026).
Conclusion: In patients with advanced HF on intermittent inotropic therapy, a high DE efficiency is associated with a higher risk of mortality or HF hospitalization in a 12-month follow-up period.
期刊介绍:
The journal is aimed at clinicians and researchers from the cardiovascular disease field and will be a forum for all views and reviews relating to this discipline.Topics covered will include: ·arteriosclerosis ·cardiomyopathies ·coronary artery disease ·diabetes ·heart failure ·hypertension ·metabolic syndrome ·obesity ·peripheral arterial disease ·stroke ·arrhythmias ·genetics


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


