{"title":"外用类固醇引起的医源性库欣综合征。","authors":"Vivek Arya, Ashish Sharma, Mohammad Ali","doi":"10.5152/eurjrheum.2021.20154","DOIUrl":null,"url":null,"abstract":"A 38-year-old man presented to our hospital with reddish marks over his abdomen and swelling over his face. He was known to have extensive psoriasis with psoriatic arthritis for 5 years. Therefore, he had been using over-the-counter analgesics and a topical preparation of clobetasol. His physical examination was remarkable with rounded appearance of the face (“moon” facies), “buffalo hump” over the nape of the neck, and large red striae over the abdomen (Figure 1a). Scaly plaques of psoriasis were present over his limbs, scalp, and back (psoriasis area and severity index [PASI]: 26.1). Examination of his nails revealed brown “oil-drop” pigmentation (Figure 1b). There was tenderness over the tibial tuberosities and heels; both the knee joints had synovitis. Investigations showed an erythrocyte sedimentation rate 54 of mm/h and C-reactive protein level of 22 mg/L. His hemogram and liver and kidney function test results were normal; he received a negative test result for human leukocyte antigen-B27. Radiograph of the pelvis showed normal sacroiliac joints. His X-ray scans of the cervical, thoracic, and lumbar spine were normal. A diagnosis of psoriasis and psoriatic arthritis with iatrogenic Cushingoid features was made, and he was treated with a dose of methotrexate 20 mg weekly and apremilast 30 mg twice daily. At follow-up after 6 months, there was a significant improvement in psoriasis (PASI: 1.7), synovitis, and enthesitis, and acute-phase reactants had normalized. However, there was no significant change in the “oil-drop” pigmentation.","PeriodicalId":12066,"journal":{"name":"European journal of rheumatology","volume":null,"pages":null},"PeriodicalIF":1.3000,"publicationDate":"2022-04-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/e5/09/ejr-9-2-106.PMC10176223.pdf","citationCount":"0","resultStr":"{\"title\":\"Iatrogenic Cushing's syndrome from topical steroid use.\",\"authors\":\"Vivek Arya, Ashish Sharma, Mohammad Ali\",\"doi\":\"10.5152/eurjrheum.2021.20154\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"A 38-year-old man presented to our hospital with reddish marks over his abdomen and swelling over his face. He was known to have extensive psoriasis with psoriatic arthritis for 5 years. Therefore, he had been using over-the-counter analgesics and a topical preparation of clobetasol. His physical examination was remarkable with rounded appearance of the face (“moon” facies), “buffalo hump” over the nape of the neck, and large red striae over the abdomen (Figure 1a). Scaly plaques of psoriasis were present over his limbs, scalp, and back (psoriasis area and severity index [PASI]: 26.1). Examination of his nails revealed brown “oil-drop” pigmentation (Figure 1b). There was tenderness over the tibial tuberosities and heels; both the knee joints had synovitis. Investigations showed an erythrocyte sedimentation rate 54 of mm/h and C-reactive protein level of 22 mg/L. His hemogram and liver and kidney function test results were normal; he received a negative test result for human leukocyte antigen-B27. Radiograph of the pelvis showed normal sacroiliac joints. His X-ray scans of the cervical, thoracic, and lumbar spine were normal. A diagnosis of psoriasis and psoriatic arthritis with iatrogenic Cushingoid features was made, and he was treated with a dose of methotrexate 20 mg weekly and apremilast 30 mg twice daily. At follow-up after 6 months, there was a significant improvement in psoriasis (PASI: 1.7), synovitis, and enthesitis, and acute-phase reactants had normalized. However, there was no significant change in the “oil-drop” pigmentation.\",\"PeriodicalId\":12066,\"journal\":{\"name\":\"European journal of rheumatology\",\"volume\":null,\"pages\":null},\"PeriodicalIF\":1.3000,\"publicationDate\":\"2022-04-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/e5/09/ejr-9-2-106.PMC10176223.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"European journal of rheumatology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.5152/eurjrheum.2021.20154\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q4\",\"JCRName\":\"RHEUMATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"European journal of rheumatology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5152/eurjrheum.2021.20154","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"RHEUMATOLOGY","Score":null,"Total":0}
Iatrogenic Cushing's syndrome from topical steroid use.
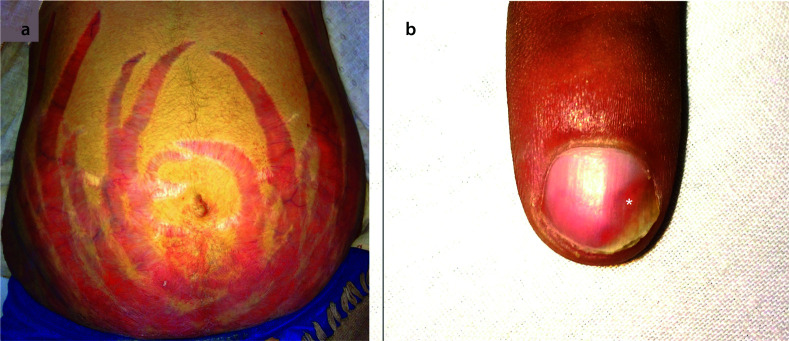
A 38-year-old man presented to our hospital with reddish marks over his abdomen and swelling over his face. He was known to have extensive psoriasis with psoriatic arthritis for 5 years. Therefore, he had been using over-the-counter analgesics and a topical preparation of clobetasol. His physical examination was remarkable with rounded appearance of the face (“moon” facies), “buffalo hump” over the nape of the neck, and large red striae over the abdomen (Figure 1a). Scaly plaques of psoriasis were present over his limbs, scalp, and back (psoriasis area and severity index [PASI]: 26.1). Examination of his nails revealed brown “oil-drop” pigmentation (Figure 1b). There was tenderness over the tibial tuberosities and heels; both the knee joints had synovitis. Investigations showed an erythrocyte sedimentation rate 54 of mm/h and C-reactive protein level of 22 mg/L. His hemogram and liver and kidney function test results were normal; he received a negative test result for human leukocyte antigen-B27. Radiograph of the pelvis showed normal sacroiliac joints. His X-ray scans of the cervical, thoracic, and lumbar spine were normal. A diagnosis of psoriasis and psoriatic arthritis with iatrogenic Cushingoid features was made, and he was treated with a dose of methotrexate 20 mg weekly and apremilast 30 mg twice daily. At follow-up after 6 months, there was a significant improvement in psoriasis (PASI: 1.7), synovitis, and enthesitis, and acute-phase reactants had normalized. However, there was no significant change in the “oil-drop” pigmentation.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


