{"title":"滑液检查发现色素绒毛碎片。","authors":"Ufuk İlgen, Hakan Emmungil","doi":"10.5152/eurjrheum.2021.20152","DOIUrl":null,"url":null,"abstract":"A 55-year-old woman with no systemic disease presented to our hospital with unilateral knee swelling for 3 years. The swelling was progressive in nature, with acute exacerbations. Physical examination revealed painless moderate joint effusion with no accompanying arthritic features clinically. Aspiration yielded a slightly turbid yellow fluid, with 3,500 white blood cells/mm3 (60% polymorphonuclear cells). No crystals were found in the sediment examination, and no bacteria were identified on Gram staining. Bacterial cultures were also negative. She had moderate effusion and synovial hypertrophy with no Doppler signal in the suprapatellar recess on ultrasonography. Plain radiography was unremarkable. Acute-phase reactants were normal, and she was negative for rheumatoid factor, anti-cyclic citrullinated peptide, and anti-nuclear antibodies. A dose of triamcinolone hexacetonide 40 mg was administered intra-articularly for a diagnosis of chronic undifferentiated monoarthritis. She presented with a huge effusion in the same joint 2 months later. Synovial fluid examination was similar, except that she had pigmented synovial villus fragments on microscopy (Figure 1). Magnetic resonance imaging showed effusion and synovial thickening with villus-like projections primarily localized in the suprapatellar recess, iso/hypointense T1and T2-weighted images with hypointense foci, and diffuse gadolinium enhancement (Figure 2). These findings were suggestive of pigmented villonodular synovitis. An open synovectomy was performed. Pathological examination revealed hyperplastic synovium with papillary projections containing hemosiderin-laden macrophages, foamy histiocytes, and multinucleated giant cells, which confirmed the diagnosis. The patient is being followed up with no relapse. Ufuk İlgen, Hakan Emmungil Images in Rheumatology","PeriodicalId":12066,"journal":{"name":"European journal of rheumatology","volume":"9 2","pages":"104-105"},"PeriodicalIF":1.3000,"publicationDate":"2022-04-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/0d/47/ejr-9-2-104.PMC10176224.pdf","citationCount":"0","resultStr":"{\"title\":\"Pigmented villus fragments on synovial fluid examination.\",\"authors\":\"Ufuk İlgen, Hakan Emmungil\",\"doi\":\"10.5152/eurjrheum.2021.20152\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"A 55-year-old woman with no systemic disease presented to our hospital with unilateral knee swelling for 3 years. The swelling was progressive in nature, with acute exacerbations. Physical examination revealed painless moderate joint effusion with no accompanying arthritic features clinically. Aspiration yielded a slightly turbid yellow fluid, with 3,500 white blood cells/mm3 (60% polymorphonuclear cells). No crystals were found in the sediment examination, and no bacteria were identified on Gram staining. Bacterial cultures were also negative. She had moderate effusion and synovial hypertrophy with no Doppler signal in the suprapatellar recess on ultrasonography. Plain radiography was unremarkable. Acute-phase reactants were normal, and she was negative for rheumatoid factor, anti-cyclic citrullinated peptide, and anti-nuclear antibodies. A dose of triamcinolone hexacetonide 40 mg was administered intra-articularly for a diagnosis of chronic undifferentiated monoarthritis. She presented with a huge effusion in the same joint 2 months later. Synovial fluid examination was similar, except that she had pigmented synovial villus fragments on microscopy (Figure 1). Magnetic resonance imaging showed effusion and synovial thickening with villus-like projections primarily localized in the suprapatellar recess, iso/hypointense T1and T2-weighted images with hypointense foci, and diffuse gadolinium enhancement (Figure 2). These findings were suggestive of pigmented villonodular synovitis. An open synovectomy was performed. Pathological examination revealed hyperplastic synovium with papillary projections containing hemosiderin-laden macrophages, foamy histiocytes, and multinucleated giant cells, which confirmed the diagnosis. The patient is being followed up with no relapse. Ufuk İlgen, Hakan Emmungil Images in Rheumatology\",\"PeriodicalId\":12066,\"journal\":{\"name\":\"European journal of rheumatology\",\"volume\":\"9 2\",\"pages\":\"104-105\"},\"PeriodicalIF\":1.3000,\"publicationDate\":\"2022-04-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/0d/47/ejr-9-2-104.PMC10176224.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"European journal of rheumatology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.5152/eurjrheum.2021.20152\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q4\",\"JCRName\":\"RHEUMATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"European journal of rheumatology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5152/eurjrheum.2021.20152","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"RHEUMATOLOGY","Score":null,"Total":0}
Pigmented villus fragments on synovial fluid examination.
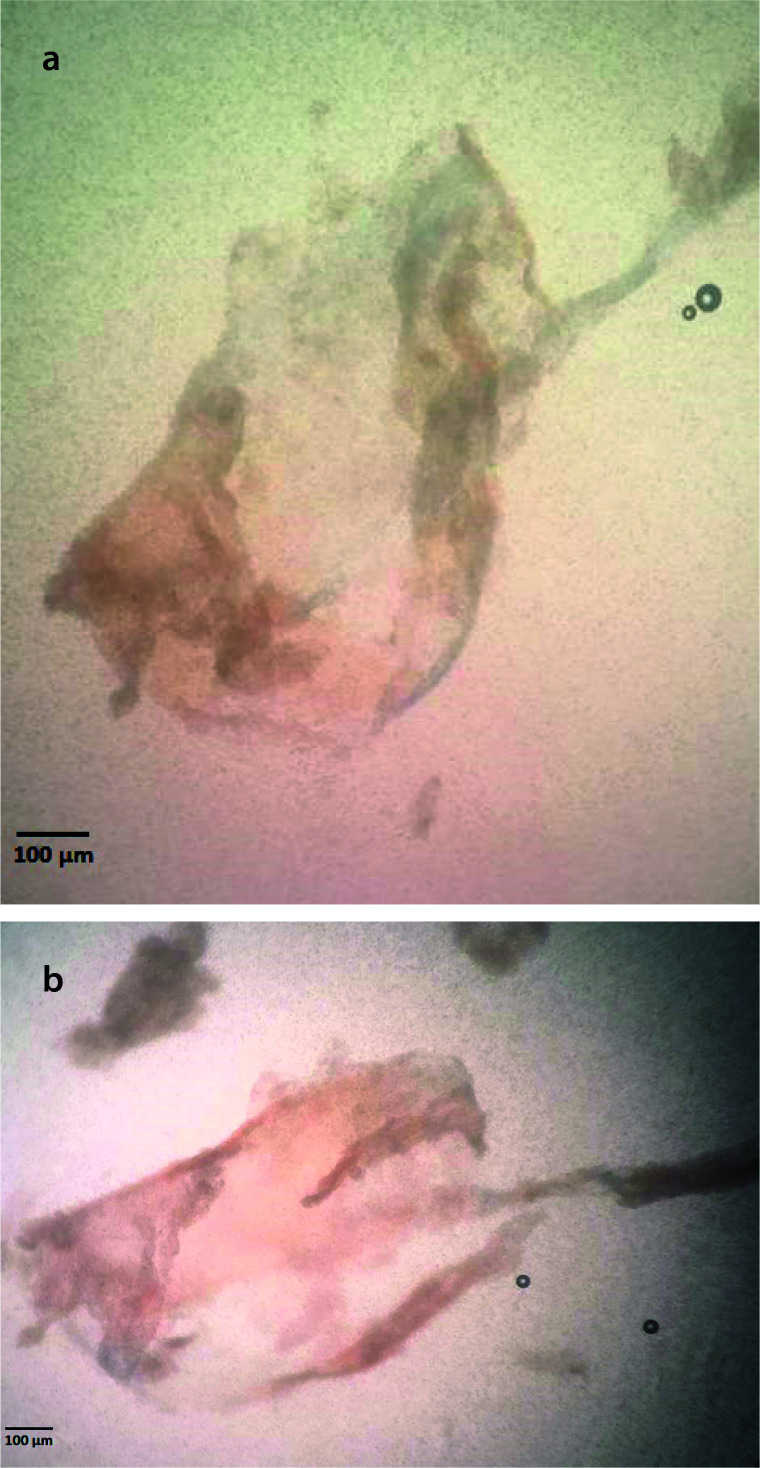
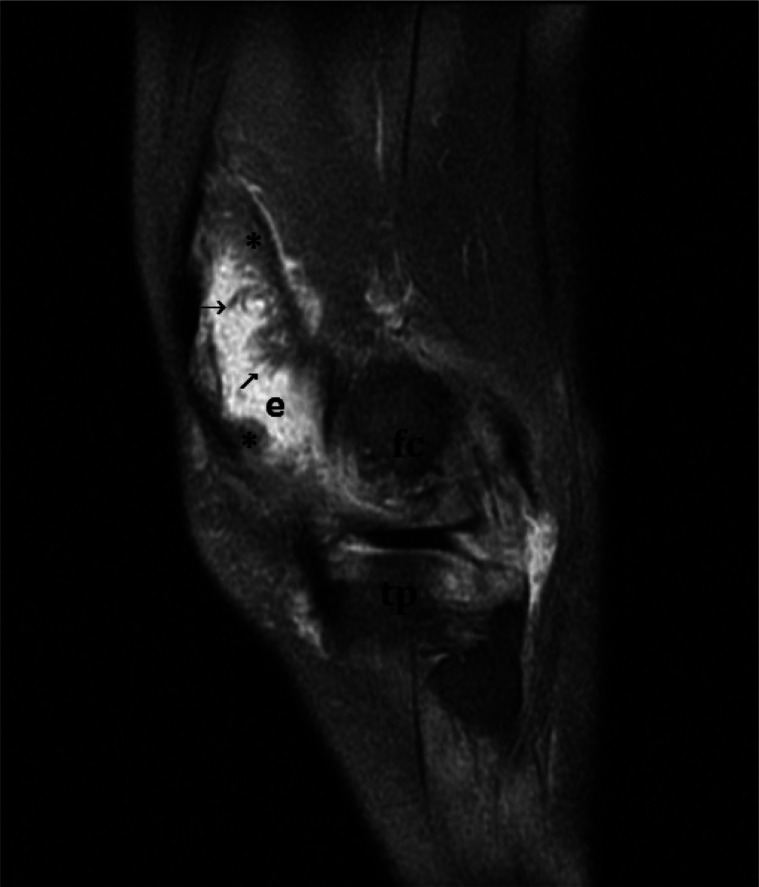
A 55-year-old woman with no systemic disease presented to our hospital with unilateral knee swelling for 3 years. The swelling was progressive in nature, with acute exacerbations. Physical examination revealed painless moderate joint effusion with no accompanying arthritic features clinically. Aspiration yielded a slightly turbid yellow fluid, with 3,500 white blood cells/mm3 (60% polymorphonuclear cells). No crystals were found in the sediment examination, and no bacteria were identified on Gram staining. Bacterial cultures were also negative. She had moderate effusion and synovial hypertrophy with no Doppler signal in the suprapatellar recess on ultrasonography. Plain radiography was unremarkable. Acute-phase reactants were normal, and she was negative for rheumatoid factor, anti-cyclic citrullinated peptide, and anti-nuclear antibodies. A dose of triamcinolone hexacetonide 40 mg was administered intra-articularly for a diagnosis of chronic undifferentiated monoarthritis. She presented with a huge effusion in the same joint 2 months later. Synovial fluid examination was similar, except that she had pigmented synovial villus fragments on microscopy (Figure 1). Magnetic resonance imaging showed effusion and synovial thickening with villus-like projections primarily localized in the suprapatellar recess, iso/hypointense T1and T2-weighted images with hypointense foci, and diffuse gadolinium enhancement (Figure 2). These findings were suggestive of pigmented villonodular synovitis. An open synovectomy was performed. Pathological examination revealed hyperplastic synovium with papillary projections containing hemosiderin-laden macrophages, foamy histiocytes, and multinucleated giant cells, which confirmed the diagnosis. The patient is being followed up with no relapse. Ufuk İlgen, Hakan Emmungil Images in Rheumatology


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


