{"title":"肠系膜上动脉综合征是术后难治性呕吐的罕见原因:1例报告。","authors":"Sanketh Edem, Aakansha Giri Goswami, Bibek Karki, Preeti Acharya, Udit Chauhan, Navin Kumar, Somprakas Basu","doi":"10.2147/CEG.S416391","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Superior mesenteric artery syndrome is a very rare cause of proximal intestinal obstruction. The objective of this clinical case report is to highlight that this unusual condition can occur in the early postoperative period and medical management may completely cure the condition.</p><p><strong>Clinical case: </strong>A middle-aged female who was being treated for pulmonary tuberculosis underwent exploratory laparotomy with limited ileal resection and a loop ileostomy for multiple ileal perforations. Postoperatively, she was restarted on anti-tubercular drugs (ATD) but developed a drug reaction, recurrent bilious vomiting, and jaundice and ATD had to be stopped. But her vomiting did not abate and she progressively developed septicemia. An abdominal CT scan diagnosed Wilkie's syndrome, and she was managed non-operatively by decubitus, parenteral nutrition, and nasojejunal tube feeding supplemented with prokinetics and antibiotics. But her sepsis did not resolve. Intraoperative histopathology suggested Candida infection, and she recovered only after systemic antifungal therapy.</p><p><strong>Discussion: </strong>Debilitation conditions like tuberculosis cause weight loss and loss of intra-abdominal fat pad, which is known to precipitate SMA syndrome. However, its presentation in the early post-operative period is rare. Symptoms may vary from non-specific abdominal fullness and weight loss to features of acute bowel obstruction. CECT of whole abdomen can help in confirming the diagnosis. SMA syndrome is often not considered in differential diagnosis and can delay treatment. Medical management is the mainstay treatment option, although surgery is reserved for cases, which fail medical treatment.</p><p><strong>Conclusion: </strong>High suspicion is needed to diagnose SMA syndrome in the postoperative period, which precipitates with intractable bilious vomiting. Medical management may be curative. The precipitating factor for SMA syndrome should also be addressed to improve the overall patient outcome.</p>","PeriodicalId":10208,"journal":{"name":"Clinical and Experimental Gastroenterology","volume":"16 ","pages":"101-105"},"PeriodicalIF":2.5000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/33/57/ceg-16-101.PMC10318104.pdf","citationCount":"0","resultStr":"{\"title\":\"Superior Mesenteric Artery Syndrome as a Rare Cause of Postoperative Intractable Vomiting: A Case Report.\",\"authors\":\"Sanketh Edem, Aakansha Giri Goswami, Bibek Karki, Preeti Acharya, Udit Chauhan, Navin Kumar, Somprakas Basu\",\"doi\":\"10.2147/CEG.S416391\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Superior mesenteric artery syndrome is a very rare cause of proximal intestinal obstruction. The objective of this clinical case report is to highlight that this unusual condition can occur in the early postoperative period and medical management may completely cure the condition.</p><p><strong>Clinical case: </strong>A middle-aged female who was being treated for pulmonary tuberculosis underwent exploratory laparotomy with limited ileal resection and a loop ileostomy for multiple ileal perforations. Postoperatively, she was restarted on anti-tubercular drugs (ATD) but developed a drug reaction, recurrent bilious vomiting, and jaundice and ATD had to be stopped. But her vomiting did not abate and she progressively developed septicemia. An abdominal CT scan diagnosed Wilkie's syndrome, and she was managed non-operatively by decubitus, parenteral nutrition, and nasojejunal tube feeding supplemented with prokinetics and antibiotics. But her sepsis did not resolve. Intraoperative histopathology suggested Candida infection, and she recovered only after systemic antifungal therapy.</p><p><strong>Discussion: </strong>Debilitation conditions like tuberculosis cause weight loss and loss of intra-abdominal fat pad, which is known to precipitate SMA syndrome. However, its presentation in the early post-operative period is rare. Symptoms may vary from non-specific abdominal fullness and weight loss to features of acute bowel obstruction. CECT of whole abdomen can help in confirming the diagnosis. SMA syndrome is often not considered in differential diagnosis and can delay treatment. Medical management is the mainstay treatment option, although surgery is reserved for cases, which fail medical treatment.</p><p><strong>Conclusion: </strong>High suspicion is needed to diagnose SMA syndrome in the postoperative period, which precipitates with intractable bilious vomiting. Medical management may be curative. The precipitating factor for SMA syndrome should also be addressed to improve the overall patient outcome.</p>\",\"PeriodicalId\":10208,\"journal\":{\"name\":\"Clinical and Experimental Gastroenterology\",\"volume\":\"16 \",\"pages\":\"101-105\"},\"PeriodicalIF\":2.5000,\"publicationDate\":\"2023-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/33/57/ceg-16-101.PMC10318104.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical and Experimental Gastroenterology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.2147/CEG.S416391\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical and Experimental Gastroenterology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2147/CEG.S416391","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
Superior Mesenteric Artery Syndrome as a Rare Cause of Postoperative Intractable Vomiting: A Case Report.
Background: Superior mesenteric artery syndrome is a very rare cause of proximal intestinal obstruction. The objective of this clinical case report is to highlight that this unusual condition can occur in the early postoperative period and medical management may completely cure the condition.
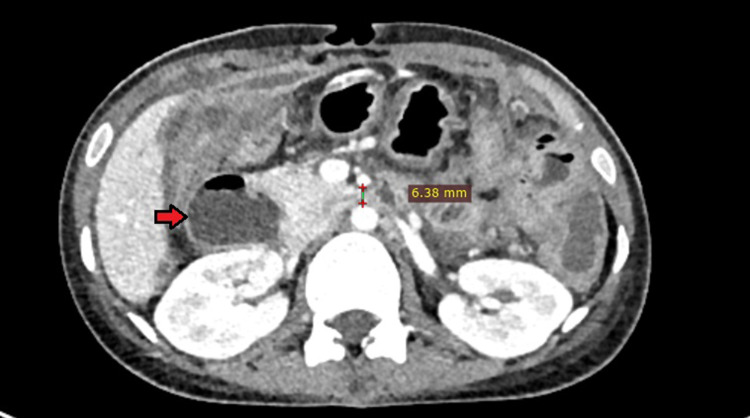
Clinical case: A middle-aged female who was being treated for pulmonary tuberculosis underwent exploratory laparotomy with limited ileal resection and a loop ileostomy for multiple ileal perforations. Postoperatively, she was restarted on anti-tubercular drugs (ATD) but developed a drug reaction, recurrent bilious vomiting, and jaundice and ATD had to be stopped. But her vomiting did not abate and she progressively developed septicemia. An abdominal CT scan diagnosed Wilkie's syndrome, and she was managed non-operatively by decubitus, parenteral nutrition, and nasojejunal tube feeding supplemented with prokinetics and antibiotics. But her sepsis did not resolve. Intraoperative histopathology suggested Candida infection, and she recovered only after systemic antifungal therapy.
Discussion: Debilitation conditions like tuberculosis cause weight loss and loss of intra-abdominal fat pad, which is known to precipitate SMA syndrome. However, its presentation in the early post-operative period is rare. Symptoms may vary from non-specific abdominal fullness and weight loss to features of acute bowel obstruction. CECT of whole abdomen can help in confirming the diagnosis. SMA syndrome is often not considered in differential diagnosis and can delay treatment. Medical management is the mainstay treatment option, although surgery is reserved for cases, which fail medical treatment.
Conclusion: High suspicion is needed to diagnose SMA syndrome in the postoperative period, which precipitates with intractable bilious vomiting. Medical management may be curative. The precipitating factor for SMA syndrome should also be addressed to improve the overall patient outcome.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


