Anouk Rijken, Vincent C J van de Vlasakker, Geert A Simkens, Koen P Rovers, Felice N van Erning, Miriam Koopman, Cornelis Verhoef, Johannes H W de Wilt, Ignace H J T de Hingh
{"title":"在一项全国性队列研究中,原发性肿瘤切除或全身治疗作为孤立的同步结直肠癌腹膜转移患者的姑息性治疗。","authors":"Anouk Rijken, Vincent C J van de Vlasakker, Geert A Simkens, Koen P Rovers, Felice N van Erning, Miriam Koopman, Cornelis Verhoef, Johannes H W de Wilt, Ignace H J T de Hingh","doi":"10.1007/s10585-023-10212-y","DOIUrl":null,"url":null,"abstract":"<p><p>Limited data are available to guide the decision-making process for clinicians and their patients regarding palliative treatment options for patients with isolated synchronous colorectal cancer peritoneal metastases (CRC-PM). Therefore, the aim of this study is to analyze the outcome of the different palliative treatments for these patients. All patients diagnosed with isolated synchronous CRC-PM between 2009 and 2020 (Netherlands Cancer Registry) who underwent palliative treatment were included. Patients who underwent emergency surgery or curative intent treatment were excluded. Patients were categorized into upfront palliative primary tumor resection (with or without additional systemic treatment) or palliative systemic treatment only. Overall survival (OS) was compared between both groups and multivariable cox regression analysis was performed. Of 1031 included patients, 364 (35%) patients underwent primary tumor resection and 667 (65%) patients received systemic treatment only. Sixty-day mortality was 9% in the primary tumor resection group and 5% in the systemic treatment group (P = 0.007). OS was 13.8 months in the primary tumor resection group and 10.3 months in the systemic treatment group (P < 0.001). Multivariable analysis showed that primary tumor resection was associated with improved OS (HR 0.68; 95%CI 0.57-0.81; P < 0.001). Palliative primary tumor resection appeared to be associated with improved survival compared to palliative systemic treatment alone in patients with isolated synchronous CRC-PM despite a higher 60-day mortality. This finding must be interpreted with care as residual bias probably played a significant role. Nevertheless, this option may be considered in the decision-making process by clinicians and their patients.</p>","PeriodicalId":10267,"journal":{"name":"Clinical & Experimental Metastasis","volume":"40 4","pages":"289-298"},"PeriodicalIF":4.2000,"publicationDate":"2023-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10338565/pdf/","citationCount":"0","resultStr":"{\"title\":\"Primary tumor resection or systemic treatment as palliative treatment for patients with isolated synchronous colorectal cancer peritoneal metastases in a nationwide cohort study.\",\"authors\":\"Anouk Rijken, Vincent C J van de Vlasakker, Geert A Simkens, Koen P Rovers, Felice N van Erning, Miriam Koopman, Cornelis Verhoef, Johannes H W de Wilt, Ignace H J T de Hingh\",\"doi\":\"10.1007/s10585-023-10212-y\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Limited data are available to guide the decision-making process for clinicians and their patients regarding palliative treatment options for patients with isolated synchronous colorectal cancer peritoneal metastases (CRC-PM). Therefore, the aim of this study is to analyze the outcome of the different palliative treatments for these patients. All patients diagnosed with isolated synchronous CRC-PM between 2009 and 2020 (Netherlands Cancer Registry) who underwent palliative treatment were included. Patients who underwent emergency surgery or curative intent treatment were excluded. Patients were categorized into upfront palliative primary tumor resection (with or without additional systemic treatment) or palliative systemic treatment only. Overall survival (OS) was compared between both groups and multivariable cox regression analysis was performed. Of 1031 included patients, 364 (35%) patients underwent primary tumor resection and 667 (65%) patients received systemic treatment only. Sixty-day mortality was 9% in the primary tumor resection group and 5% in the systemic treatment group (P = 0.007). OS was 13.8 months in the primary tumor resection group and 10.3 months in the systemic treatment group (P < 0.001). Multivariable analysis showed that primary tumor resection was associated with improved OS (HR 0.68; 95%CI 0.57-0.81; P < 0.001). Palliative primary tumor resection appeared to be associated with improved survival compared to palliative systemic treatment alone in patients with isolated synchronous CRC-PM despite a higher 60-day mortality. This finding must be interpreted with care as residual bias probably played a significant role. Nevertheless, this option may be considered in the decision-making process by clinicians and their patients.</p>\",\"PeriodicalId\":10267,\"journal\":{\"name\":\"Clinical & Experimental Metastasis\",\"volume\":\"40 4\",\"pages\":\"289-298\"},\"PeriodicalIF\":4.2000,\"publicationDate\":\"2023-08-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10338565/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical & Experimental Metastasis\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1007/s10585-023-10212-y\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"ONCOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical & Experimental Metastasis","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s10585-023-10212-y","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"ONCOLOGY","Score":null,"Total":0}
Primary tumor resection or systemic treatment as palliative treatment for patients with isolated synchronous colorectal cancer peritoneal metastases in a nationwide cohort study.
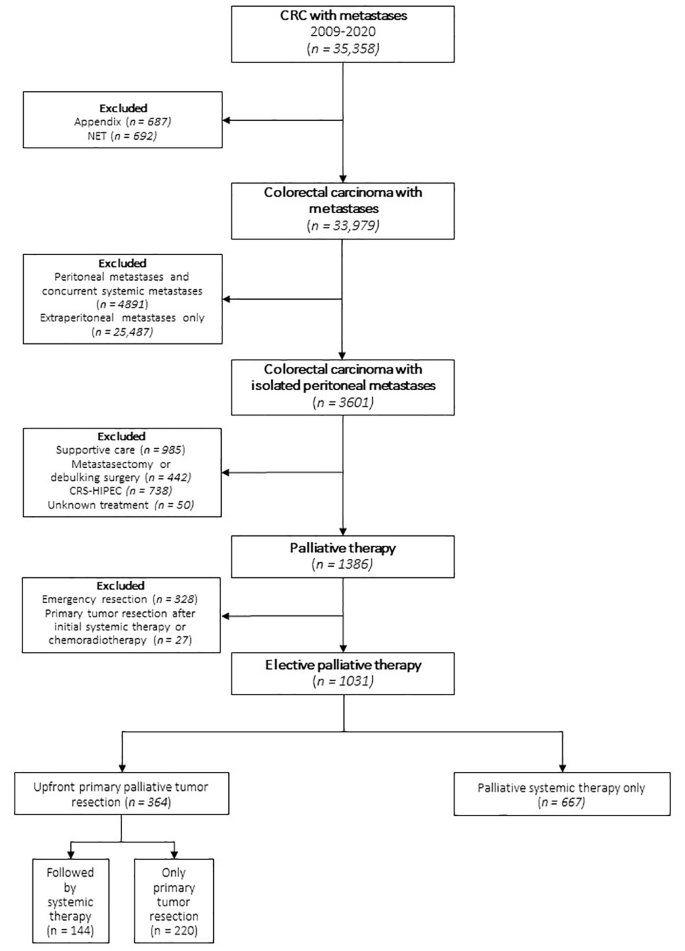
Limited data are available to guide the decision-making process for clinicians and their patients regarding palliative treatment options for patients with isolated synchronous colorectal cancer peritoneal metastases (CRC-PM). Therefore, the aim of this study is to analyze the outcome of the different palliative treatments for these patients. All patients diagnosed with isolated synchronous CRC-PM between 2009 and 2020 (Netherlands Cancer Registry) who underwent palliative treatment were included. Patients who underwent emergency surgery or curative intent treatment were excluded. Patients were categorized into upfront palliative primary tumor resection (with or without additional systemic treatment) or palliative systemic treatment only. Overall survival (OS) was compared between both groups and multivariable cox regression analysis was performed. Of 1031 included patients, 364 (35%) patients underwent primary tumor resection and 667 (65%) patients received systemic treatment only. Sixty-day mortality was 9% in the primary tumor resection group and 5% in the systemic treatment group (P = 0.007). OS was 13.8 months in the primary tumor resection group and 10.3 months in the systemic treatment group (P < 0.001). Multivariable analysis showed that primary tumor resection was associated with improved OS (HR 0.68; 95%CI 0.57-0.81; P < 0.001). Palliative primary tumor resection appeared to be associated with improved survival compared to palliative systemic treatment alone in patients with isolated synchronous CRC-PM despite a higher 60-day mortality. This finding must be interpreted with care as residual bias probably played a significant role. Nevertheless, this option may be considered in the decision-making process by clinicians and their patients.
期刊介绍:
The Journal''s scope encompasses all aspects of metastasis research, whether laboratory-based, experimental or clinical and therapeutic. It covers such areas as molecular biology, pharmacology, tumor biology, and clinical cancer treatment (with all its subdivisions of surgery, chemotherapy and radio-therapy as well as pathology and epidemiology) insofar as these disciplines are concerned with the Journal''s core subject of metastasis formation, prevention and treatment.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


